7: Promoting Good Health and Wellness
- Last updated
- Save as PDF
- Page ID
- 69634

Learning Objectives
By the end of this chapter, you should be able to:
- Summarize what goes into child and staff health records.
- Describe the process of daily health checks.
- Explain good dental hygiene practices in the classroom.
- Discuss the importance of sleep.
- Identify different screenings early care and education programs can implement.
- Relate the importance of developmental screening.
- Recall ways to engage families in the screening process.
|
|
Licensing RegulationsTitle 22 Regulations that relate to this chapter include: 101220 CHILD’S MEDICAL ASSESSMENTS
101220.1 IMMUNIZATIONS
101221 CHILD’S RECORDS
101226.1 DAILY INSPECTION FOR ILLNESS
|
Introduction
Healthy development continues to support learning throughout childhood and later life. “Health in the earliest years…lays the groundwork for a lifetime of well-being…”303 To promote the health of children in early care and education programs, it’s important to keep records of both children's and staff’s health. Programs can support children’s oral health and healthy sleep habits. And they can help identify developmental and health concerns with screening.

Children’s Health Records
“The health and safety of individual children requires that information regarding each child in care be kept and available when needed. Children’s records consist of various documentation such as a child’s medical and immunization history, emergency medical care information, and parental permission to participate in specific activities…Each child care facility must keep accurate records on each child receiving care in child care.”305
Health records can help early care and education programs identify preventative health measures, develop care plans for children with special needs, and determine whether or not a child should be excluded from care due to illness.
California Title 22 Child Care licensing requirements list the following health-related items to include in the child’s records:
- Medical assessment and the following health information:
- Dietary restrictions and allergies.
- Instructions for action to be taken in case the child's authorized representative, or the physician designated by the authorized representative, cannot be reached in an emergency.
- A signed consent form for emergency medical treatment
- Record of any illness or injury requiring treatment by a physician or dentist and for which the center provided assistance to the child in meeting his/her necessary medical or dental needs.
- Record of current medications, including the name of the prescribing physician, and instructions, if any, regarding control and custody of medications.
- Current and updated immunization records306
The National Health and Safety Standards recommends that the following also be included in the child’s records:
- A health history completed by the family at admission
- The child’s health insurance information307

Staff Health Records
It is also important for records to be kept to document the health of all staff in an early care and education program. Licensing requires the following health-related items to be in staff records:
- Health Screening Report
- TB Clearance309
In September of 2016, Senate Bill 792 was passed that requires staff or volunteers in an early care and education program to provide records of immunizations (or immunity) for
- Pertussis
- Measles
- Influenza (annually between August 1 and December 1 of each year; can decline in writing)310
|
|
The Importance of Keeping Staff Healthy A culture of wellness is a working environment where an employee's health and safety is valued, supported, and promoted through worksite, health and wellness programs, policies, benefits, and environmental supports. A culture of wellness for staff is really going to be the foundation for creating a culture of health and safety for children. Staff have health problems such as obesity and depression at rates above the national average. Early care and education salaries are often low, creating personal financial stress. Staff turnover rates are high. In general, early childhood educators are undervalued for the important and high-demand work they do. Staff wellness and stability will affect the quality of services a program is able to deliver to families and children. Children need consistent, sensitive, caring, and stable relationships with adults. Adults who are well, physically and mentally, are more likely to engage in positive relationships. When we support staff well-being, we strengthen early care and education. Programs can use the CDC’s Workplace Health Model to support the health of their staff.311 It is outlined in this image (and a link is provided in the Further Resources to Explore feature at the end of the chapter). 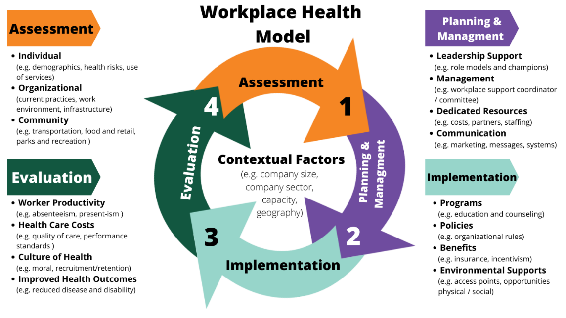
planning and management, implementation, and evaluation.312 |
|
|
Pause to Reflect What does staying healthy mean to you? What do you do (or could you do) to manage your stress, reinforce your resilience, and keep yourself physically healthy (nutrition, activity, etc.)? How could your employer help you stay healthy? |
Daily Health Checks
Every day an informal, observation-based quick health check should be performed on every child (before the parent/caregiver leaves). Early childhood educators should use their knowledge about what is normal for a child to identify any concerns about the child’s well-being (but not as an attempt to formally diagnose illness). It is not a process that formally excludes children from illness, but following up concerns noticed at a health check may find reasons to exclude children.
“In a child care setting where lots of people are coming at the same time, it is hard to take a moment with each child. However, this welcoming routine can establish many things and is a good child development policy. This contact will help [teachers] better understand each child, help the children feel comfortable and good about themselves, reduce the spread of illness by excluding children with obvious signs of illness, and foster better communications with [families].”313

Conducting the Daily Health Check
Teachers should use all of their senses to check for signs of illness. This includes:
- Listening to what families tell you about how their child is feeling and what the child sounds like (hoarse voice, coughing, wheezing, etc.)
- Looking at the child from head to toe (with a quick scan) to see if the child looks flushed, pale, has a rash, has a runny nose or mucus in the eyes
- Feeling the child’s cheek or neck (as part of a greeting) for warmth or clamminess
- Smelling the child for unusual smelling breath or a bowel movement.
Here are the signs to observe for:
- General mood and atypical behavior
- Fever (elevated temperature)
- Rashes or unusual spots, itching, swelling, and bruising
- Complaints of not feeling well
- Symptoms of illness (coughing, sneezing, runny nose, eye or ear discharge, diarrhea, vomiting, etc.)
- Reported illness in child or family members315,316
Dental Hygiene
Dental hygiene is important to prevent Early Childhood Caries (ECC), which is a term used to describe tooth decay, including filled or extracted teeth due to decay, in the primary teeth (baby teeth). It is important to rethink the way we “treat” dental caries. Traditionally, we would wait until a child had a cavity and “treat” the cavity with a filling. In order to prevent ECC, we must intervene before the first cavity develops.317 Early care and education programs can teach children and families about dental hygiene and oral care as well as implement good dental hygiene practices. Here are some ideas:
- Use teaching practices that engage children and promoting thinking critically. Consider asking questions such as:
- How do you brush your teeth?
- Why do you brush your teeth?
- What else can you do to keep your mouth and teeth healthy?
- What happens if you don’t brush your teeth?
- Tell me about your last visit to the dentist.
- Integrate oral health into activities (in addition to tooth brushing). Some possibilities include:
- Having children separate pictures of foods that are good for oral health from pictures of foods that are high in sugar.
- Reading books with positive oral health messages to children.
- Having children pretend they are visiting a dental office.
- Singing songs about oral health
- Engage families in promoting oral health at home. Some ways to do this include:
- Working with families to find the best ways to position their child for tooth brushing. Remind families that young children cannot brush their teeth well until age 7 to 8. It is also important for a parent to brush their child’s teeth or help them with brushing.
- Asking families to take photographs of their child brushing his teeth and helping the child write stories about his experience.
- Helping families choose and prepare foods that promote good oral health.
- Encouraging families to ask their child what she learned about oral health in school that day.
- Offering families suggestions for at-home activities that support what children are learning about oral health at school.318
Classroom Tooth Brushing Steps
- Sitting at a table in a circle, children brush teeth as a group activity every day.
- Give each child a small paper cup, a paper towel, and a soft-bristled, child-sized toothbrush.
- Put a small (pea-sized) dab of fluoride toothpaste on the inside rim of each cup, and have children use their toothbrushes to pick up the dabs of toothpaste.
- Brush together for two minutes, using an egg timer or a song that lasts for about two minutes.
- Brush your teeth with the children to set an example, and remind them to brush all of their teeth, on all sides.
- When the two minutes are up, have the children spit any extra toothpaste into their cups, wipe their mouths and throw the cups and paper towels away.
- Children can go to the sink in groups to rinse their toothbrushes and put the toothbrushes in holders to dry.319

Sleep Hygiene
It's important to get enough sleep. Sleep supports mind and body health. Getting enough sleep isn’t only about total hours of sleep. It’s also important to get good quality sleep on a regular schedule to feel rested upon waking.
Sleep is an important part of life! Young children spend around half of their time asleep.321
- Babies need to sleep between 12 and 16 hours a day (including naps).
- Toddlers need to sleep between 11 and 14 hours a day (including naps).
- Preschoolers need to sleep between 10 and 13 hours a day (including naps).
- School-aged children need 9 to 12 hours of sleep each night.322
We know how busy they are when they are awake, but what are they doing during all of those restful hours? Actually, sleep has many purposes.
- Growth: Growth hormone is released when children sleep (Berk 2002, 302). Young children are growing in their sleep, and since they have a lot of growing to do, they need all the sleep they can get.
- Restoration: Some sleep researchers have found that sleep is important for letting the brain relax and restore some of the hormones and nutrients it needs (Jenni & O’Conner 1995, 205).
- Memory: Sleep is also a time when the brain is figuring out what experiences from the day are important to remember (Jenni & O’Conner 1995, 205).
- Health: One study found that infants and toddlers need at least 12 hours of sleep in a 24 hour day. When infants and toddlers had less than 12 hours they were more likely to be obese by the age of 3 (Taveras et. al. 2008, 305).323
The Culture of Sleep and Child Care
Across the world people sleep in different ways. Some people sleep inside, some sleep outside. Some people sleep in beds, others in hammocks or on mats on the floor. Some people sleep alone, some sleep with a spouse or children or both. Some people sleep only at night, while others value a nap during the day. How, when, and where people choose to sleep has a lot to do with their culture, traditions, and customs. This can include where they live, how their family sleeps, even how many bedrooms are in their home. Teachers have a role in providing a sleep environment that is comfortable and safe for the children in their care, while honoring families’ cultural beliefs.
What can teachers do to help young children feel more “at home” when it is time for them to rest?
- Think of sleep and sleep routines as part of the child’s individualized curriculum.
- Classroom teachers should meet with a family before a child enters your care. This is an opportunity to find out about a child’s sleep habits before they join the classroom. When you know how a baby sleeps at home, you can use that information to plan for how they might sleep best in your care.
- Brainstorm ways to adapt your classroom to help a child feel “at home” during rest times. For example, a baby who is used to sleeping in a busy environment might nap better if you roll a crib into the classroom. Some mobile infants and toddlers might have a hard time sleeping in child care because they think they will miss something fun! These children benefit from having a very quiet place to fall asleep. When you have a positive relationship with a baby it will be easier to know what will help them relax into sleep.
- Encourage families to bring in “a little bit of home” to the program – like a stuffed animal or special blanket. A comfort item from home can help children feel connected to their families. They might want that comfort all day. The comfort item from home can also help children make the transition to sleep while in your care. Make sure that infants under one year of age do not have any extra toys or blankets in the crib with them.
- Share with families what you learn about their child. Use pick up and drop off times to ask questions about sleep at home. Families can share information that could make their child more comfortable in your care. You can be a resource for families about sleep and their child. Remember that families are the experts about their child.
Napping and Individual Differences
Have you noticed that some children will fall asleep every day at the same time no matter what else is going on? These kids could fall asleep into their lunch if it is served too late! Have you known children who seem to fall asleep easily some days and other times just can’t settle into sleep? These children might need a very stable routine. Some toddlers nap less and sleep more at night while others need to have a long sleep during the day.
Temperament and Sleep
Some of the different patterns in children’s sleep has to do with their temperament (Jenni & O’Connor 2005, 204). Temperament is like the personality we are born with. Some children are naturally easy-going and adapt to new situations while others really need a routine that is the same every day. One child might fall asleep easily just by putting her in her crib or cot when she is drifting off to sleep. Another child might fall asleep in your arms but startle awake the moment he realizes he has been laid down alone.
Circadian Rhythms and Sleep
Something else that can make nap time easy or difficult for young children has to do with their natural sleep cycles. Everyone has a kind of “clock” inside of their bodies that tells them when they are hungry or sleepy. The cycle of this clock is called circadian rhythms. Circadian rhythms are the patterns of sleeping, waking, eating, body temperature and even hormone releases in your body over a twenty-four hour period. How much children need to sleep, when they feel tired, and how easily they can fall asleep are all related to their circadian rhythms (Ferber 2006, 31).
Meeting Each Individual Child’s Sleep Needs
Thinking about the circadian rhythms and temperament reminds us how each child is different. That is why it is important to have nap times that meet the needs of all children in your care. Helping young children to learn to recognize their bodies’ needs and find ways to meet those needs is the very important skill of self-regulation.324

|
|
Individualizing Nap Schedules Creating a space for sleepy children can allow them to relax or nap when their body tells them they are tired. It can take some creativity to figure out how to let a young child nap or rest when they are tired. What do you do if a child won’t nap when others are? How does one child rest quietly in a busy classroom? Two-and-a-half-year-old Henry is new to your classroom. His mother has shared with you that he does not nap during the day with her. When nap time comes around you can tell that Henry does not seem very tired. What can you do for Henry, or other children like him, while the rest of the class sleeps?
|
Developmental and Health Screenings
There are specific health conditions that impact learning and development, which can be identified and treated early. These conditions can be identified through early health screening.327
Screening is the first step in getting to know a child at the beginning of each enrollment year. This "baseline data" helps staff plan and individualize services. It also helps them identify "red flags" for further examination or evaluation. When concerns go unidentified, they can lead to bigger problems.328
Screening helps staff and families:
- Celebrate milestones: Every family looks forward to seeing a child’s first smile, first step, and first words. Regular screenings with early childhood professionals help raise awareness of a child’s development, making it easier to celebrate developmental milestones.
- Promote universal screening: All children need support in the early years to stay healthy and happy. Just like regular hearing and vision screenings can assure that children are able to hear and see clearly, developmental and behavioral screenings can assure that children are making progress in areas such as language, social, or motor development.
- Identify possible delays and concerns early: With regular screenings, families, teachers, and other professionals can assure that young children get the services and supports they need as early as possible to help them thrive.
- Enhance developmental supports: Families are children’s first and most important teachers. Tools, guidance, and tips recommended by experts, can help families support their children's development.329
Screening is part of a larger process professionals use to learn about children's health and development. In partnership with families, developmental monitoring (or surveillance), screening, and assessment keep children on track developmentally.
|
|
What is the Difference Between Screening, Assessment, and Evaluation Screening The screening process is the preliminary step to determine if sensory, behavioral, and development skills are progressing as expected. The screening itself does not determine a diagnosis or need for early intervention. Assessment Assessment is an on-going process to determine a child’s and family’s strengths and needs. The assessment process should be continued throughout a child’s eligibility and be used to determine strategies to support the development of the child in the classroom and at home. This can be both a formal or informal process. Evaluation A formal evaluation is performed by a qualified professional to identify or diagnose a developmental, sensory, or behavioral condition or disability requiring intervention. Only children who were identified through screening and ongoing assessment as possibly having a condition or disability might require intervention. The Early Intervention Part C agency or Local Education Agency in your community must be notified for a formal evaluation to determine his or her eligibility for early intervention, special education or other related services.330 |
A couple of important things to remember about screening:
- Children develop rapidly during the first three years of life, so keeping a watchful eye on health and development for infants and toddlers is critical.
- Most early childhood programs serve diverse families. Therefore, the best screening tools gather information in ways that respond to culture and language.331
- Developmental screening using research-based standardized developmental screening instruments that are valid and reliable for the population and purpose for which they will be used; age, developmentally, culturally, and linguistically appropriate, and appropriate for children with disabilities, as needed; and conducted by qualified and trained personnel. Currently, standardized screening instruments for children birth to age 5 are widely available in English and Spanish, but are virtually unavailable for children whose families speak other languages.332
|
|
Engaging Families in Screening and Follow-UpFamilies can be your most powerful ally and asset throughout the screening process. They are the expert on their child and can provide meaningful and reliable information. Screenings are also an opportunity to support families to focus on their child and increase their understanding of their child’s development. When families are active partners in the assessment (and intervention) process, staff and families are able to share an understanding of what is best for the child, the families ' priorities, and goals for the child’s learning and development. You can engage families by:
|
Developmental Monitoring and Screening
The first years of life are so important for a child’s development. Early experiences make a difference in how young children’s brains develop and can influence lifelong learning and health. Early childhood educators spend a great deal of time with young children and are instrumental in determining many of the kinds of experiences they will have. Developmental monitoring means observing and noting specific ways a child plays, learns, speaks, acts, and moves every day, in an ongoing way. Developmental monitoring often involves tracking a child’s development using a checklist of developmental milestones.
Teachers are in a unique position to monitor the development of each child in their care. They may be the first one to observe potential delays in a child’s development. Working with groups of same-aged children can help teachers recognize children who reach milestones early and late. Working with children of different ages can help teachers notice if a child’s skills are more similar to those of a younger or older child than to those of his or her same-aged peers. Because teachers spend their day teaching, playing with, and watching children, they may find themselves concerned that a child in their care is not reaching milestones that other children his or her age have, or they may have families ask them if they are concerned about their child’s development. 334
|
|
The first time I heard the term “developmental monitoring,” I was really intimidated and thought, “this sounds really complicated and time-consuming. How am I going to do that on top of everything else I have to do during the day?” I was so relieved when I found out that “developmental monitoring” is just a fancy way of saying “watch, observe and record what the kids are doing to make sure they’re on track.” I just mark on a simple checklist when children meet milestones. We observe children every day anyway. We watch what they’re doing when they play in the classroom or outside, when they eat, and so on. Monitoring is just that: watching and observing, and recording what you see. Making a check on a list when a child meets a milestone takes about two seconds, and it’s easier than just about anything else we do all day. It’s definitely easier than getting a room full of toddlers to sleep at naptime, and it’s a lot more fun than changing diapers! And if that’s all it takes to really make sure each child is on track and to make sure I’m not missing anything in all the hubbub each day, I’m all over it! -Ms. Carolyn (an early childhood educator)335 |
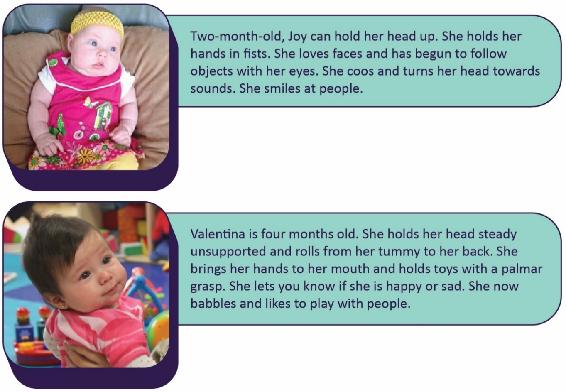
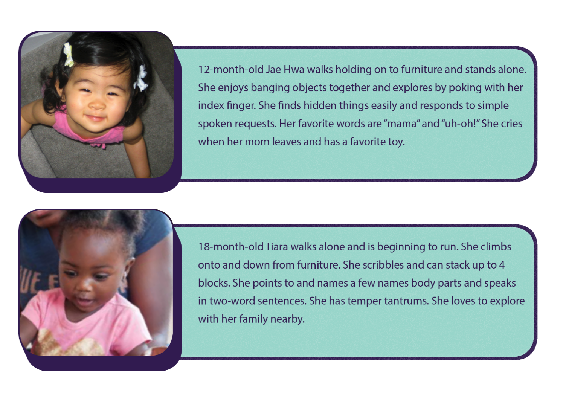
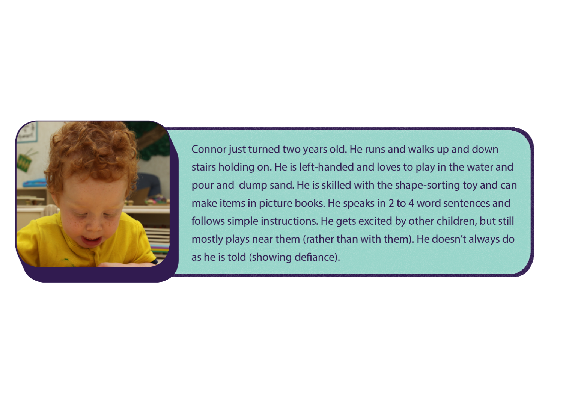
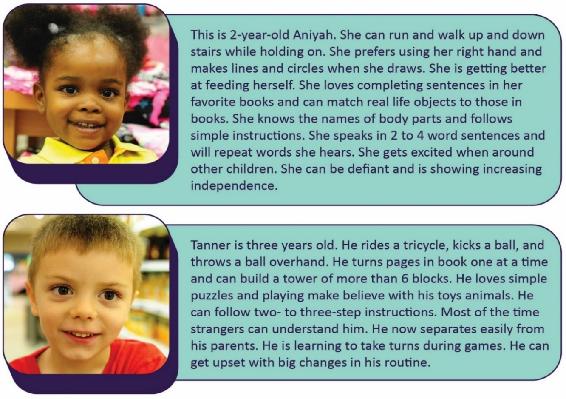
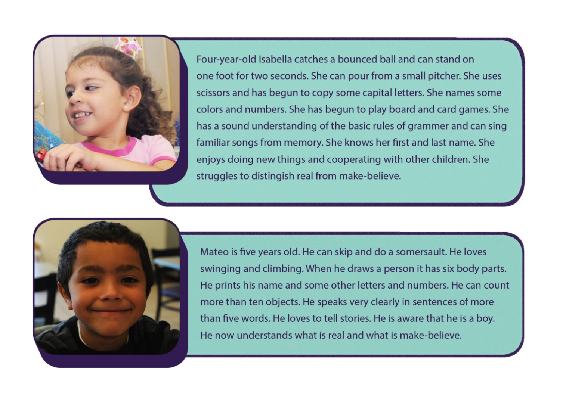
A complete list of developmental milestones for children from birth to age 8 is in Appendix I, but here are some examples of children birth to age 5 that showcase typical milestones for their age.

|
|
Pause to ReflectDo you feel like you are less knowledgeable about or have less experience with a specific age of children (refer to Appendix I to see detailed milestones from 2 months through 12 years of age)? What can you do to improve your familiarity with the milestones for children that age? Why would this be important? |
Developmental screening is a more formal process that uses a validated screening tool at specific ages to determine if a child's development is on track or whether he or she needs to be referred for further evaluation.337
Screening alone is not enough to identify a developmental concern. Rather, it helps staff and families decide whether to refer a child for more evaluation by a qualified professional. The earlier a possible delay is identified, the earlier a program can refer a child for further evaluation and additional supports and services.338
Most children with developmental delays are not identified early enough for them to benefit from early intervention services; early care and education programs can help change that. Although about 1 in 6 children has a developmental disability, less than half of these children are identified as having a problem before starting school.
Too often, adults don’t recognize the signs of a potential developmental disability, they are not sure if their concern is warranted, or they don’t have resources to help make their concern easier to talk about. But pinpointing concerns and talking about them is very important to get a child the help he or she might need.339
Developmental screening involves:
- Research-based, standardized developmental screening tools
- Information from family members, teachers, and other staff who know the child
- Written parental consent before starting the screening
- Communication with families in their home language
Appropriate Screening Tools
When searching for screening tools, keep the following in mind.
- Screening tools must be research-based and designed to be a brief measure of development that identifies if the child needs a more in-depth evaluation.
- Screening tools should be
- Age-appropriate
- Culturally appropriate
- Sensitive to the family's home language
- Used by trained and qualified personnel
- Valid for the intended results
- Reliable across users
- Clearly identified for use in screening
Programs need to make careful and informed decisions about whether to screen a child who is a dual language learner (DLL) in their home language, English, or both. Some skills may look different depending on the child's culture and background. Use a screening tool that considers the child's cultural context. When a culturally appropriate screening tool is not available, asking families about their child's typical behavior becomes even more critical. This information helps staff interpret screening results.
Timing
Programs should complete the first developmental screening in the first month or two of care. Programs may keep track of a child's development with an annual screening after that. Also, a child and family's primary health care provider may do developmental screening, autism spectrum disorder screening, and developmental surveillance.
After Screening
These are examples of the next steps a program might take based on the results of the screening.
Results: There are no concerns.
Action: The child participates in ongoing, individualized care. Staff do ongoing child assessments.
Results: The results are unclear or there may be additional concerns.
Action: The child participates in ongoing, individualized care. Staff do ongoing child assessments. The family and staff closely observe the child's development over time to decide if they should re-screen or evaluate the child.
Results: The screening or information collected from family members, teachers, and other program staff found some concerns.
Action: The child participates in ongoing, individualized care. Program staff work with the family to refer the child for a free evaluation. Infants and toddlers go to the appropriate Individuals with Disabilities Education Act (IDEA) Part C agency and preschool children go to the appropriate Part B agency, usually a school district. Families may need support to navigate the referral and evaluation process.340
If a delay or disability is diagnosed, early treatment is important. Speech therapy, physical therapy, and other services are available in every state for free or at low cost to families. However, if a developmental concern is not identified early, families can't take advantage of these services.341
Vision Screening
Families and early care and education staff cannot always tell when a child has trouble seeing. Observation alone isn’t enough. This is why implementing evidence-based vision screening throughout early childhood is important.
Timely vision screening (coupled with an eye examination2 when indicated) is an important step toward early detection of any possible vision problems. Early detection can lead to an effective intervention and help to restore proper vision. Young children rarely complain when they can’t see well because to them, it’s normal.
Engaging Families
It is easier for families to partner with early care and education staff and health care providers when they understand how vision influences their child’s development and learning. Preparing families about what to expect from a vision screening helps them know how to prepare their child. It is also important to talk about who will have access to their child’s screening results. One of the best ways to promote children’s vision health is by developing and implementing policies and procedures that both define and support ways for staff to collaborate with families.
Include questions on the program’s family health history form to identify children who may have a higher risk of vision problems. For example is there a family history of amblyopia, strabismus, or early and serious eye disease?
Provide resources to help families learn more about healthy eyes and the importance of early detection of vision problems. Do families know that it isn’t always possible to tell if children have a vision problem just by looking at their eyes? Or that young children seldom complain when they can’t see well?
In addition to assuring timely vision screening, programs can support children and families who have been given treatment recommendations from an eye specialist (such as wearing glasses or patching one eye for amblyopia), as well as reminding families of follow-up visits to the eye doctor whenever recommended.

Rescreening
Programs that perform vision screenings will need to determine when to rescreen children who do not pass. Some children may be unable to pay attention, cooperate or understand what they need to do during the first attempt at screening. This is especially true for visual acuity testing. These children may not have “failed” their vision screening. They may be considered “untestable.”
Research shows that preschool children who are “untestable” are almost twice as likely to have a vision problem as those who successfully pass a screening. They should be rescreened as soon as possible, but not longer than 6 months later. If a child fails or is untestable at the second attempt, consider referring the child for a full eye examination.
Ongoing Care
It is important to remember that screening only provides a vision assessment at one moment in time. Occasionally a family member or teacher will identify a new or different vision concern after a child has been previously screened. In addition, as children grow their eyes change and new signs of an eye problem or blurred vision can arise as they mature. Programs should address this new concern with the parent and the health care provider promptly.343
Hearing Screening
Families and early care and education staff cannot always tell when a child is deaf or hard of hearing. Observation alone isn’t enough. This is why implementing evidence-based hearing screening throughout early childhood is important.
Hearing helps us communicate with others and understand the world around us. However, about 2 to 3 of every 1,000 children in the United States are born deaf or hard of hearing. A child may also experience a decline in hearing ability at any time caused by illness, physical trauma, or environmental or genetic factors. It is estimated that the incidence of permanent hearing loss doubles by the time children enter school. A child may have difficulty hearing in one ear or both ears. The difficulty may be temporary or permanent. It may be mild or it may be a complete inability to hear spoken language and other important sounds.
Any inability to hear clearly can get in the way of a child’s speech, language, social and emotional development, and school readiness. Intervention may improve social and emotional and academic achievement when children who are deaf or hard of hearing are identified early.

An evidence-based hearing screening is a way to identify children who need an evaluation to determine if they are deaf or hard of hearing. Prior to discharge from the hospital, almost all newborns are screened and an evaluation is necessary for those who do not pass the screening.
Engaging Families
It is easier for families to partner with early care and education staff and health care providers when they understand how hearing influences their child’s speech and language development, socialization, and learning. Preparing families about what to expect from a hearing screening helps them know how to prepare their child. It is also important to talk about who will have access to their child’s screening results. When a child does not pass a hearing screening, programs can provide support to help families follow up with referrals and any recommended treatment. If a child is identified as deaf or hard of hearing, collaboration between the family, the early care and education program, and the child’s audiologist and other early intervention providers will be helpful. Share information with the family about the importance of hearing for children’s language development and communication. This supports a family’s health literacy, and it may help them complete the follow-up steps.
Rescreening
If your program performs a hearing screening and a child does not pass, it is important for you to collaborate with and support the family to complete all recommended follow-up steps.
- The child is typically screened a second time within about 2 weeks.
- If the child does not pass, the child should be referred to a health care provider for a middle ear evaluation. A health care provider can diagnose and treat common problems such as earwax buildup or middle ear infections. A third screening is necessary after the medical examination.
- If a child still does not pass, programs should recommend for a referral to a pediatric audiologist for a complete diagnostic evaluation.
It is also important for programs to support families to follow up if the program obtains results from the child’s health care provider indicating that the child did not pass a hearing screening.345
|
|
Pause to ReflectDo you remember getting your vision or hearing screened during your childhood? If you were diagnosed with vision or hearing impairments, how was it discovered? At what age did that happen? |
Lead Screening
Lead screening measures the level of lead in the blood. Lead is a poison that is very dangerous for young children because of their small size and rapid growth and development. It can cause anemia, learning difficulties, and other medical problems.
Children can inhale or swallow lead through exposure to:
- Home or child care environments, including those:
- Built before 1960 with peeling paint or renovation
- Located near a highway or lead industry
- Family members who work with lead or have been treated for lead poisoning
- Imported ceramic pottery for cooking, storing, or serving food
- Home remedies with lead
- Certain candies, which may contain high levels of lead in the wrapper or stick. Be cautious when providing imported candies to children.
- Eating paint chips or dirt
- Water pumped through lead-based pipes
Lead screening involves a blood lead test, from a finger stick or a venous blood draw. It is recommended at 12 months and 24 months of age. Children from 3 to 6 years of age should have their blood tested if they have not been tested
Symptoms of Lead Poisoning
Most children with lead poisoning show no symptoms. However, you might notice:
- Developmental delay
- Learning Difficulties
- Irritability
- Headaches
- Poor appetite or stomachache
- Weight loss
- Fatigue and sluggishness
- Slow growth and development
- Vomiting
- Constipation
- Hearing loss
Follow-Up to Lead Screening
New recommendations from the Centers for Disease Control and Prevention (CDC) state that if screening indicates a lead level of five micrograms per deciliter or more, the child should be referred to a health professional. 346
Lead has negative outcomes on a variety of things, including:
- Attention (easily distracted, challenges with sustained attention, hyperactivity)
- executive functions (problems with planning, impulse control, flexible thinking, etc.)
- visual-spatial skills (problems related to visual perception, memory, organization, and reasoning with visually presented information)
- social behavior (aggression, disruptive behavior, poor self-regulation)
- speech and language (problems with phonological and sentence processing and spoken word recognition)
- fine and gross motor skills (unsteadiness, clumsiness, and problems with coordination, visual-motor control, and dexterity)347
Depending on the effects of lead poisoning, early care and education programs can implement intervention services to support the child. Other treatments include:
- Nutrition counseling
- Iron supplements
- Medication to remove the lead from the blood
- Follow-up testing of the child's blood
- Referral for developmental testing348
Social and Emotional and Behavioral Screening
Young children are learning to get along with others and manage their own emotions. When a child enters a program, staff get to know what social and emotional skills children are working on. They can use social and emotional or behavioral screening tools to gather that information.349
support for children’s social and emotional health.350
Social and emotional health—the ability to form strong relationships, solve problems, and express and manage emotions—is critical for school readiness and lifelong success. Without it, young children are more likely to:
- Have difficulty experiencing or showing emotions, which may lead to withdrawal from social activities and maintaining distance from others
- Have trouble making friends and getting along with others
- Have behaviors, such as biting, hitting, using unkind words, or bullying—behaviors that often lead to difficulty with learning, suspension or expulsion, and later school dropout351
More information about this topic can be found in other parts of this book. Behavior has been addressed in Chapter 3 in the section on Interpersonal Safety and children’s mental health is the focus of Chapter 11.
Summary
By keeping accurate records, conducting daily health checks, supporting children’s development of good dental hygiene, and by providing for individual children’s sleep needs early care and education programs can help promote good health on a daily basis. When programs monitor and screen children, they can ensure that conditions or situations that might interfere with a child’s health or well-being can be identified and supports put in place to mitigate potential negative effects.