
6.6: Gross and Fine Motor Development
- Page ID
- 139866
Two Types of Motor Development
Motor skills are often broadly divided into gross motor and fine motor skills. Gross motor skills pertain to skills involving large muscle movements, such as independent sitting, crawling or walking. Fine motor skills involve use of smaller muscles, such as grasping, object manipulation, or drawing. [1]

Motor Milestones
Infants and toddlers are constantly learning about the world as they experience it and actively engage with it during the first three years of life. Milestones represent what most children (75% or more) can do by specific ages. This chart represents the new and improved milestone charts provided by the CDC in 2022 with substantial evidence-based updates. These milestone charts are meant to prompt surveillance and conversation and, if needed, identification and early intervention. The CDC adopts a proactive stance—we should take action early when developmental concerns arise rather than the perspective of waiting to see if a child “catches up”. While children do develop at individual paces, being proactive during these critical early years is essential (Morgan et al., 2021; Noritz et al., 2013). The chart below lists milestones that, if children are not achieving by specific ages, caregivers should encourage parents to communicate with their family’s pediatrician. Most caregivers are not professionally trained to officially assess the developmental abilities of children; however, caregivers have the ability to track developmental progress and are often the first to notice developmental concerns. Here is a table of some of the motor milestones for infants and toddlers.
|
Age |
What Most Children Can Do By Each Age [3] |
|---|---|
|
2 months |
● Hold their head up when on their tummy. ● Move both arms and both legs. ● Open hands briefly. |
|
4 months |
● Hold their head steady without support while being held. |
|
6 months |
● Roll from tummy to back. |
|
9 months |
● Stand while holding on for support. ● Can get into a sitting position. ● Sit without support. ● Pull up into a standing position. ● Crawl. |
|
12 months |
● Pull up to stand. |
| 15 months |
● Take a few steps independently. ● Use fingers to feed themselves some food. |
|
18 months |
● Walk without holding on to anyone or anything. ● Scribble. ● Drink from a cup without a lid and may spill sometimes. ● Feed themselves with their fingers. ● Try to use a spoon. ● Climb on and off a couch or chair without help. |
|
24 months |
● Kick a ball. ● Run. ● Walk (not climb) up a few stairs with or without help. ● Eat with a spoon. |
| 30 months |
● Use their hands to twist things, like turning door knobs or unscrewing lids. |
|
36 months |
● String items together, like large beads or macaroni. |
Motor Development Concerns
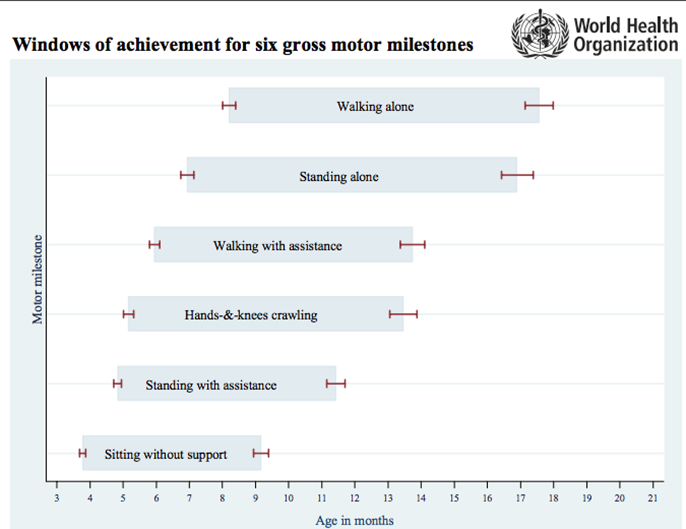
The motor milestones from the CDC are based on data from infants and toddlers in the U.S., which may not accurately represent the motor development of children from other countries (Karasik, Tamis-LeMonda, Adolph & Bornstein, 2015). Figure 6.6.2 is based on research conducted by the World Health Organization (WHO Multicentre Growth Reference Study Group, & de Onis, 2006). It presents windows of achievement for six gross motor development milestones based on infants and toddlers from five countries: Ghana, India, Norway, Oman and the USA. The six milestones in the chart are sitting without support, standing with assistance, hand and knees crawling, walking with assistance, standing alone and walking alone.
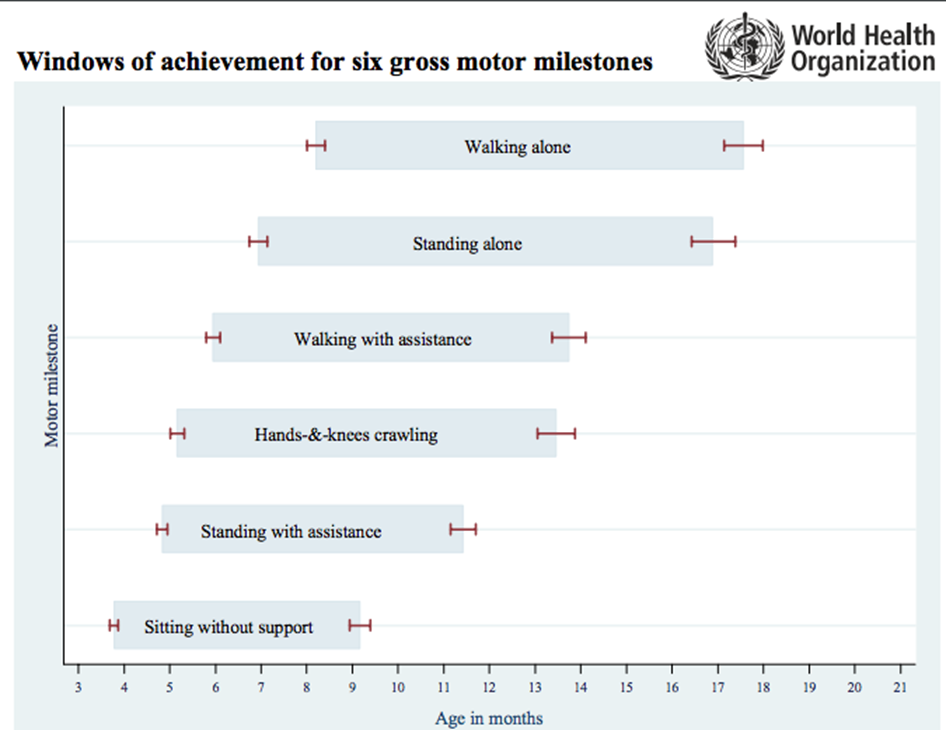
Based on the research, there are a few findings worth noting:
- In general, there is a common order in achieving these milestones. First children are able to sit without support, then achieve standing with assistance, followed by walking with assistance which then leads to standing alone and lastly walking alone.
- The one milestone that did not always follow the general order was hand-and-knees crawling. Sometimes children would crawl on their hands and knees before being able to stand with assistance.
- 4.3% of infants did not exhibit hand-and-knees crawling at all—they skipped this milestone and went straight into walking.
- The windows of achievement overlap—Figure \(\PageIndex{2}\) clearly depicts this. The start of each window of achievement for every milestone does not begin near the end of the previous milestone window, but rather begins near the beginning of the previous milestone window. This overlap acknowledges the wide age variability of infants and toddlers achieving these milestones.
- The length of each milestone window varies across the motor skills. Walking alone and standing alone have the longest achievement window, suggesting that these two abilities have the most variability in age of achievement. For example, some children began walking alone around eight months of age, while others did not achieve this milestone until after seventeen months of age. On the other hand, sitting without support and standing with assistance showed the two most narrow windows of achievement, suggesting that these two abilities have the least variability in age of achievement.
Motor Milestone Chart Limitations
Gross motor milestone charts, while important, do not capture the complex developments that lead up to achieving specific milestones. Take for example the process to be able to sit independently. The ability to maintain balance in the sitting posture gradually emerges between 2 and 9 months of age (Butler et al., 2010). When infants are 5 to 6 months old, they are able to ‘prop sit’ or sit independently for short periods (Shumway-Cook & Woollacott, 2003). At 6 months, hip joint mobility increases, allowing the thighs to rest on the contact surface and the infant is able to sit with their legs in a ring position (Bly, 1994), i.e., symmetrically flexed, abducted with externally rotated hips and flexed knees. Between 8 to 9 months, the trunk and pelvis muscles stabilize the sitting position, allowing the infant to narrow the support base for balanced independent sitting (Harbourne, Lobo, Karst & Galloway, 2013; van der Fits et al., 1999). After being able to sit independently, infants learn to perform a coordinated action between upper limbs, trunk and lower limbs as they are able to use their lower body to balance as they reach with their upper limbs (Rochat & Goubet, 1995). Thus, unlike milestone charts that simply show sitting to occur, sitting without support is a process that takes place over many months and involves a complex interplay between various muscles that prepare for the eventual achievement of sitting. [5]

Another limitation of motor milestones is that they convey the idea that once an infant performs a motor milestone, like walking, that the infant has fully achieved this milestone. The reality is that motor development involves numerous bouts of successes and failures with each milestone ability. An infant that successfully walks once, may fall the very next attempt. Karen Adolph and her colleagues (2012) have documented the number of steps and falls toddlers have as they learn to walk. Toddlers between 12 to 18 months of age take an average of 2,368 steps in just one hour and cover a distance of 701 meters—the length of almost eight football fields! This is just one hour; multiplying these numbers by the total number of hours toddlers are awake is even more eye-opening. In six hours, a toddler could accumulate around 14,000 total steps and cover the distance of 46 football fields! Despite these infants clearly being able to walk, they also continue to fall. In fact, the average toddler fell seventeen times each hour, one toddler even fell sixty-nine times in one hour.

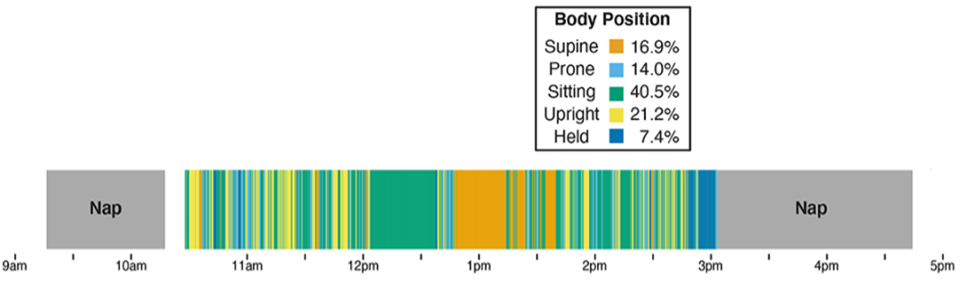
Every day, infants are practicing various motor skills and body positions. For example, Figure \(\PageIndex{5}\) provides insight into the various motor behaviors and body positions from one 10 month old infant. While the majority of time was spent in a seated position (40.5%), the infant was consistently practicing various other positions, frequently rotating between them.
Gross Motor Development
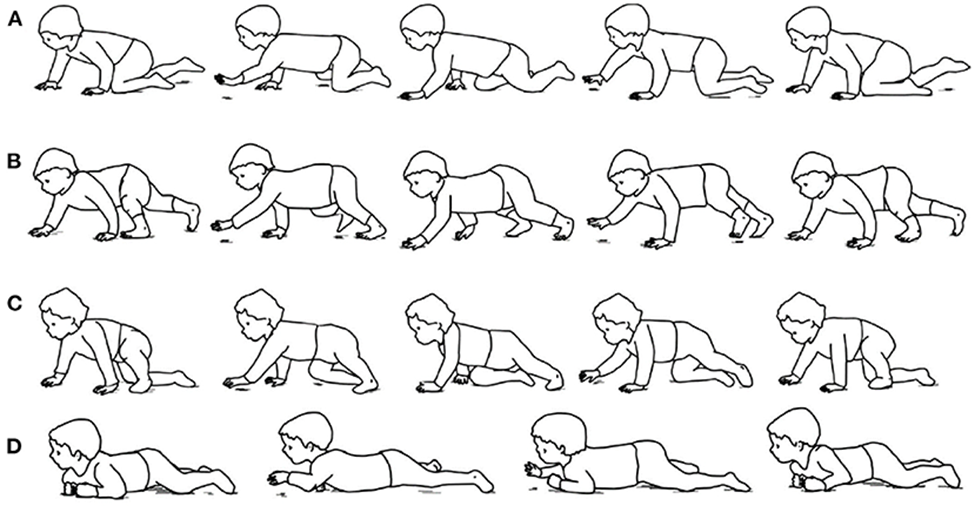
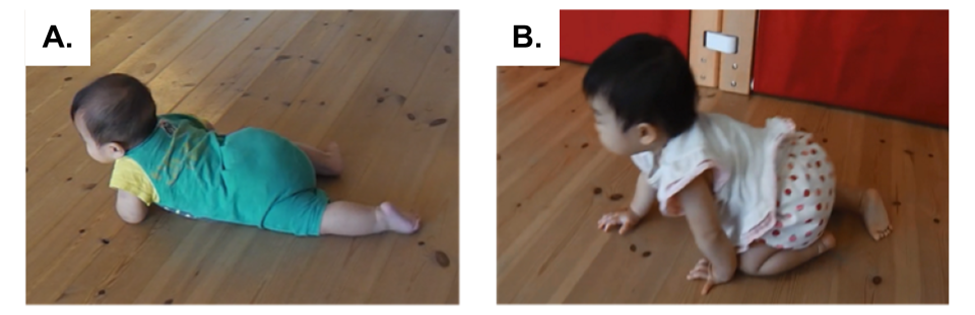
In the process of gross motor development, the first mobility that infants usually acquire is crawling. There are different types of infant crawling (see Figure \(\PageIndex{6}\) for a depiction) such as belly crawling and hands-and-knees crawling (Patrick, Noah & Yang, 2012). Belly crawling is the action in which infants move by pulling the body along the ground on the abdomen. Hands-and-knees crawling means moving by lifting the abdomen up on both arms and knees. Some infants experience both belly crawling and hands-and-knees crawling, others experience only hands-and-knees crawling (Kalmar, 2017). Previous studies have explored a relationship between belly crawling and hands-and-knees crawling: infants who formerly belly-crawled showed more proficient hands-and-knees crawling than those who skipped the belly crawling period (Adolph, Vereijken & Denny, 1998). Infants who spend a greater amount of awake time in the prone position (abdomen on ground, such as during tummy time) achieve hands-and-knees crawling at an earlier age (Davis, Moon, Sachs & Ottolini, 1998). [9]
Tummy Time.
Tummy time describes the times when a caregiver places an infant on their stomach while the infant is awake and someone is watching. Tummy time is not only an important way to prevent flat spots on a baby's head, it is also an important part of a baby's normal growth. In fact, tummy time is positively related to overall gross motor development (Buchanan et al., 2021; Carson et al., 2022; Hewitt et al., 2020). Tummy time is especially important for infants who are at risk of motor delays and/or who have a motor-related disability (Uzark et al., 2021; Wentz, 2017). While tummy time is supported by many professionals and well-respected organizations, there are arguments against the necessity of the practice (see Gerber & Johnson, 1998). [1]

Tummy time is important for many reasons:[12]
- Tummy time helps prevent flat spots on the back of an infant’s head.
- Makes neck and shoulder muscles stronger so infants can start to sit up, crawl, and walk.
- Improves infant motor skills.
Infants benefit from 2 to 3 tummy time sessions each day for a short period of time (3 to 5 minutes). As they grow and show enjoyment of tummy time, the length of the sessions can be increased. As infants grow older, more tummy time helps build strength for sitting up, rolling over, crawling, and walking. [12]
Tummy Time Tips: [12]
These suggestions can help make tummy time more enjoyable:
- Spread out a blanket in a clear area of the floor for tummy time.
- Try short tummy time sessions after a diaper change or after an infant wakes from a nap.
- Put a toy or toys within an infant's reach during tummy time to help them learn to play and interact with their surroundings.
- Have an adult be in the infant’s field of view during tummy time to encourage interaction and bonding.
- As an infant gets older, tummy time sessions can last longer, and can take place more often throughout the day.
Gross Motor Development: Postural Affordances
Postures—the particular body and limb configurations used at any moment—mediate motor development in meaningful ways (Rochat & Bullinger, 1994). For example, the acquisition of each new posture provides a unique lens through which infants can view the world as they accrue a range of motor possibilities for moving about and physically interacting with the environment (e.g., Adolph, 2008; Thurman & Corbetta, 2019). [14]
Depending on the motor skill level and posture used, physical interactions with objects can be facilitated or reduced. For example, when sitting, infants’ hands are free allowing them to manually manipulate and explore objects in sophisticated ways ( Lobo & Galloway, 2013; Lobo et al., 2014; Rochat, 1989; Soska & Adolph, 2014; Soska, Adolph & Johnson, 2010). When in a prone position (lying abdomen down), however, infants are limited to using one hand to lift their torso up off the ground, while using the other to reach out for an object, which greatly reduces the range of actions (Rocha & Tudella, 2008). In older infants, crawling and walking positions have different affordances. During crawling, infants are less likely than walking infants to carry objects (Karasik et al., 2012). In comparison, when walking, infants’ hands are free to interact with objects in complex ways and the change of position opens up a new field of view for further exploration. Thus, each posture provides unique affordances on how the body can be used (Adolph, 2008). Consider Figure \(\PageIndex{9}\) which shows an image of an infant holding an object with one hand while using the other hand for balance. In which ways does the infant’s current crawling posture afford and restrict how the infant can explore the object? If the infant transitioned into a standing or walking position, how would the affordances and restrictions change? [14]

Postures can also alter the stability of the body, the demand of attentional resources, and what can be perceived in the surroundings (Franchak, Kretch & Adolph, 2018; Kretch, Franchak & Adolph, 2014). Certain postures and their relative stability can even influence the use of the limbs and hands. For example, transitioning from sitting to crawling, and from crawling to walking affects the way infants use their arms for reaching and retrieving objects (Corbetta & Bojczyk, 2002; Corbetta & Thelen, 2002). Unstable postures often require more of the infants’ effort for balance such as when the hands are needed to hold onto surfaces during cruising (Berger, Chan & Adolph, 2014), or when the hands may be needed to balance the body when standing is a new motor skill still being learned (Ledebt, 2000). When the hands are used for balance, they are less likely to be used for holding and exploring objects. [14]
Thus, research has shown that postural progression and postural control can influence infants’ experiences with objects, people, and their wider environments. Infants’ expanding repertoire of postural skills as they acquire locomotor skills, affects their manipulatory behaviors and interactive activities with objects in their surroundings. [14]
Gross Motor Development: Environmental Affordances
Think about the physical environment where you live, how does the furniture influence where and how people stand and sit, where eating takes place, the posture and arrangement people are in when socializing, how objects like televisions, windows or fireplaces influence the structure and positioning of furniture which results in how and where people sit and orient in the room, etc. Just as the physical environment is important for considering how adults sit, stand and move about in a space, the physical environment for infants and toddlers affords various physical movement possibilities.

The theory of affordance (Gibson, 1950; 2014) represents an important theoretical framework for considering the environment’s role in supporting and encouraging physical development in infants and toddlers. In this theory, the physical environment is believed to afford or allow the child possibilities and actions. The characteristics and features of the indoor environment can therefore be hypothesized to influence children’s gross motor development. The affordances of the physical environment are what the environment offers the child. For example, a toddler’s classroom’s affordances are the physical size of the classroom, the toys and materials available, the number of peers for potential play partners, and adults who set up the play environment, ensure its overall safety, manage the day-to-day operations, and interact with the children. [17] [18]

Let’s look again at the gross motor windows of achievement for six gross motor milestones chart again (Figure \(\PageIndex{12}\)). The six milestones in the chart are sitting without support, standing with assistance, hand and knees crawling, walking with assistance, standing alone and walking alone.
([20])
For each milestone, how could the physical environment support and encourage the infant or toddler as they progress toward achieving a specific milestone? For example, consider the milestone of standing with assistance, what role could the environment have? As the child is not yet able to stand independently, they are taking advantage of structures in the environment that afford assistance in getting into a standing position and remaining upright. Therefore, structures that allow a child to hold onto and pull up are important, as are structures that can be used for support to remain standing. When an environment includes structures at a low height, it supports a child's progress toward achieving this milestone. If an environment only has high structures built for adults, the motor and movement possibilities for a child are more limited.
Caregivers should consider how both the indoor and outdoors environments afford infants and toddlers the opportunity to practice and challenge their current motor skills safely. As caregivers observe and reflect upon the motor development progress of infants and toddlers they should consider how to modify the environment to continue to support and encourage motor development. For example, for infants practicing standing with support, caregivers should ensure there are structures that can be used to help infants pull themselves up and offer continual support at an appropriate height. Outside, is the play equipment age-appropriate and supportive of gross motor development? Figure \(\PageIndex{13}\) shows two angles of the same play structure geared for toddlers. Considering the construction of it, what elements are there that can support the developmental progression of toddlers’ gross motor skills? While parts of the structure may be challenging for some toddlers, what elements are built in to support toddlers as their gross motor skills improve?

Fine Motor Development
Fine motor skills involve more exact movements of the feet, toes, hands, and fingers. While fine motor skills are slower to develop (in accordance with the proximodistal trend), remarkable progress is made in fine motor development during the first two years. In just the first few years of life, children go from having no intentional fine motor control to being able to manipulate objects to play and learn, as well as beginning to take care of themselves. [22]
Just as with gross motor milestones, there are complex developments that lead up to achieving specific fine motor milestones. Take for example the fine motor milestone of grasping an object. Reaching to grasp an object, which could be perceived as a relatively simple action, requires a complex compilation of smaller abilities working synchronously together. Successful reaching to a stimulus, whether it is located on the body or in external space, typically involves the coordination of at least two different action systems: reaching and grasping (Jeannerod, 1996). Effective reaching requires individuals not only to extend their hands to the location of an object, but to also open and orient the hand to prepare to grasp the specific object. Developmentally, research indicates that the reaching system develops before grasping (Piaget, 1952; Bruner, 1973), reflecting a proximodistal sequence in the development of grasping (Lockman & Ashmead, 1983). For example, before 4 months, infants develop the ability to extend their hand to the location of an object (Bruner & Koslowski, 1972; Piaget, 1952), but during this period the hand is often fisted when it contacts the object. By 4 months, however, infants begin to open the hand in advance of contacting the object. Likewise, with regard to self-touch, closed hand contacts prevail in the first 2 or 3 months, and open hand contacts begin to increase in frequency between 3 and 5 months (Thomas, Karl & Whishaw, 2015). [23]
Even after infants achieve the ability to reach for and grasp an object, there is still further development in this milestone that occurs. There is an improvement in reaching kinematics as 6 month-old infants develop a straight arm trajectory accompanied by fewer movements (Von Hofsten, 1991). During this phase of reaching development, there are many factors that influence arm trajectory; however, the development of postural control for maintaining stability during reaching is one of the most significant (Bertenthal & Von Hofsten, 1998). Since reaching requires “whole body engagement” (Rochat & Goubet, 1995), its achievement is highly dependent on posture. At about 3 months, when arm extensions are being replaced by goal directed reaches but upright sitting is not mastered, infant reaching is better with external support. As infants generate the ability to sit independently, reaching becomes more coordinated and they can use their body to balance as they reach outward. [24]

Development of Grasping
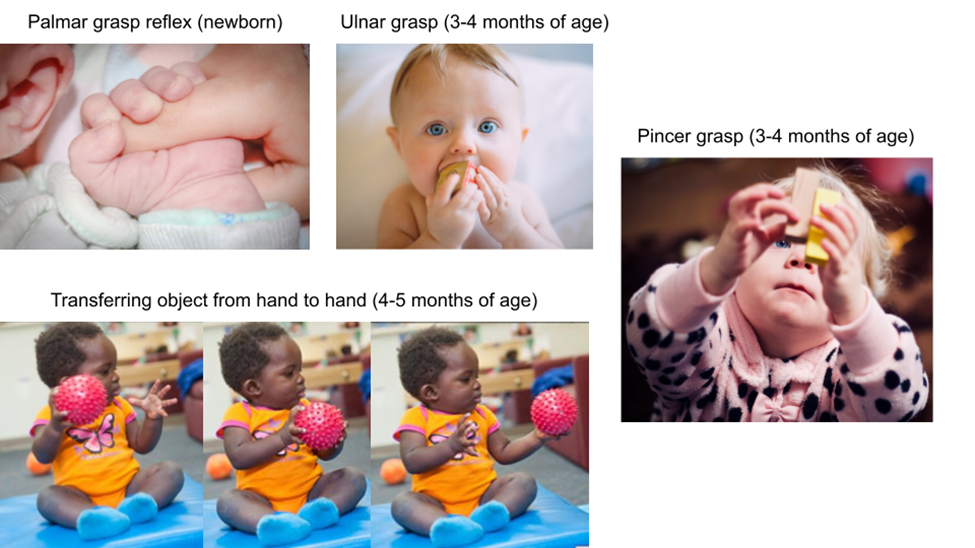
The development of grasping is an important part of fine motor development. As infants and toddlers develop, they progress through different types of grasps. Children are born with a palmar reflex grasp. It is an involuntary reflexive response present in newborns, but begins to appear around 16 weeks gestation (Sherer, 1993). To elicit the reflex, a caregiver can use their finger to stroke the palm of the infant. The palmar grasp reflex comprises two phases: finger closure and clinging. The infant's fingers undergo flexion to enclose the examiner's finger and the pressure applied to the palm produces traction on the fingers' tendons, leading to the clinging action. The thumb is not involved in this reflex. The palmar grasp reflex disappears typically by six months of age, signifying healthy brain maturation and is replaced by the development of voluntary grasping (Schott & Rossor, 2003). The palmar reflex probably serves to create a basic motor pattern that lays the foundation for obtaining later grasping ability. Additionally, it creates interaction and bonding between the infant and the caregiver. [26]
The palmar reflex grasp is replaced by the ulnar grasp, which is a “clumsy motion in which an infant’s fingers close against the palm” (Berk & Meyers, 2016). The ulnar grasp typically develops around 3 to 4 months of age and increases infants’ ability to explore objects. As infants learn to sit independently, both hands are freed up to explore objects; therefore around 4 to 5 months of age infants are able to transfer objects between their hands. The pincer grasp is when the pointer finger and the thumb squeeze together to grasp an object. Infants are usually able to perform a pincer grasp by the age of 9 to 10 months (Sgandurra et al., 2012). With each change in grasping ability, infants are able to interact with different objects and in new ways. For example, the ulnar grasp only allows for larger objects to be held onto while the pincer grasp permits an infant to pick up smaller objects.
To support infants, caregivers should carefully observe infants’ grasping progression and provide materials that can easily be manipulated based on their current grasping techniques. Active object exploration emerges around 3 to 6 months of age with the onset of reaching and grasping (Lobo & Galloway, 2008; Rochat, 1989; Ruff, 1984). At 6 months of age, infants spend the majority of their time mouthing and grasping objects and this sharply declined with concurrent improvements in complex manual exploratory behaviors such as fingering, transferring, and rotating objects (Belsky & Most, 1981; Ruff, 1984). As a result, caregivers should provide young infants with materials that they can easily grasp onto and that are safe for mouthing. Once infants begin to sit and develop more complex grasping techniques, such as the ulnar grasp, caregivers should provide materials that are more complex in design characteristics, but still light, easy to hold in one hand, easy to transfer between hands and safe for mouthing. [28]

Infant exploratory behaviors are influenced by object properties including size, shape, texture, and weight of objects. Infants change their grasping patterns depending on object size—smaller objects are grasped unimanually and larger objects are grasped bimanually. Research has demonstrated variations in infants’ grasping patterns based on object structure, such as two-handed grasps for larger objects and pincer grips for smaller and softer objects (Newell et al., 1989; Newman et al., 2001). Additionally, 12 to 14 month old infants showed appropriate, anticipatory changes in grasp formation based on object shape and size (Barrett, Traupman & Needham, 2008; Fagard, 2000). Nine to twelve month old infants explored object properties such as shape, size, and texture by rotating, fingering, and transferring objects, whereas they explored properties such as weight, sound, and rigidity by banging and shaking objects (Ruff, 1984). This research suggests that with older infants, caregivers should provide materials that are more complex in design and diverse in characteristics such as size, shape, texture and weight. As older infants use their developing grasping abilities to explore materials, caregivers can continue to observe how they interact with the materials, and provide materials based on what characteristics infants seem most interested in exploring. [28]
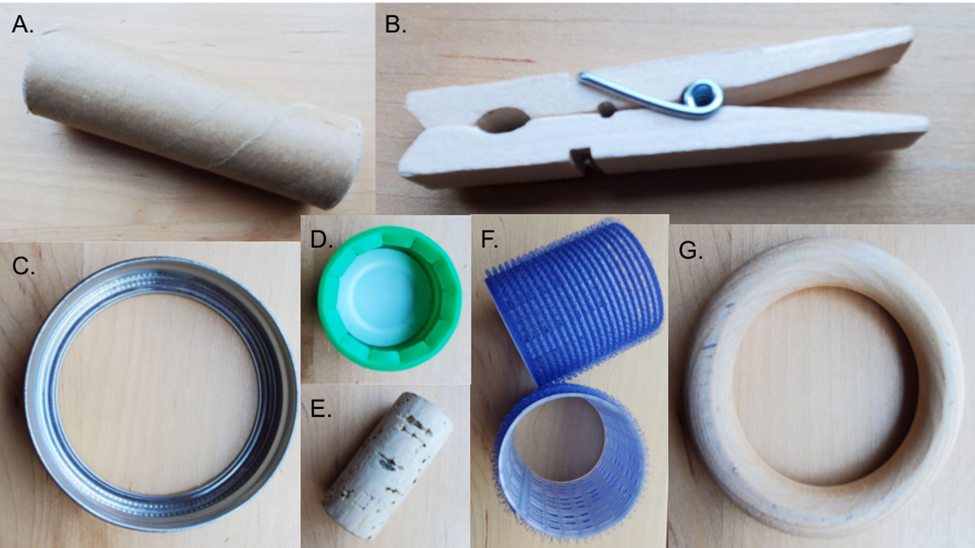
Figure \(\PageIndex{17}\) shows various manipulative objects: A) cardboard tube; B) wood clothes pin; C) metal jar lid; D) plastic bottle lid; E) cork; F) plastic hair curlers; G) wood ring. As you look over the objects, consider which objects would best support the different grasping abilities of infants? For infants using a ulnar grasp, which objects would be best to share with them? For infants using a pincer grasp, which objects would be best to share with them? How might the physical properties of each object change how the infants explore them?
[1] Gonzalez et al., (2019). Do gross and fine motor skills differentially contribute to language outcomes? A systematic review. Frontiers in Psychology, 10, 2670. CC by 4.0
[2] Image by krakenimages on Unsplash.
[3] CDC’s Developmental Milestones by the Centers for Disease Control and Prevention is in the public domain.
[4] Image from the WHO is in the public domain.
[5] Sato & Tudella (2018). Influence of sitting positions and level of trunk control during reaching movements in late preterm and full-term infants. Frontiers in Pediatrics, 6, 185. CC by 4.0
[6] Image from Juan Encalada on Unsplash.
[7] Image from julio andres rosario ortiz on Unsplash
[8] Image adapted from Franchak et al., (2021). A contactless method for measuring full-day, naturalistic motor behavior using wearable inertial sensors. Frontiers in Psychology, 4632. CC by 4.0
[9] Yamamoto et al., (2021). The applied ability in infant crawling and the importance of prone motor experience for subsequent development. Preprint. CC by 4.0
[10] Image from Xiong et al., (2021). Measurement and analysis of human infant crawling for rehabilitation: A narrative review. Frontiers in Neurology, 1747. CC by 4.0
[11] Image adapted from Yamamoto et al., (2021).The applied ability in infant crawling and the importance of prone motor experience for subsequent development. Preprint. CC by 4.0
[12] “Babies need tummy time!” from NICHD is in the public domain.
[13] Image from Minnie Zhou is on Unsplash.
[14] Thurman & Corbetta (2019). Changes in posture and interactive behaviors as infants progress from sitting to walking: a longitudinal study. Frontiers in Psychology, 10, 822. CC by 4.0
[15] Image by Minnie Zhou on Unsplash.
[16] Image from Jen Theodore on Unsplash.
[17] Sando (2019). The physical indoor environment in ECEC settings: Children’s well-being and physical activity. European Early Childhood Education Research Journal, 27(4), 506-519. CC by 4.0
[18] Stanton-Chapman & Schmidt (2021). How do the children play? The influence of playground type on children’s play styles. Frontiers in Psychology, 4337. CC by 4.0
[19] Image by Todd LaMarr is licensed under CC by 4.0
[20] Image from the WHO is in the public domain.
[21] Image by Todd LaMarr is licensed under CC by 4.0
[22] “Child Growth and Development” by College of the Canyons, Jennifer Paris, Antoinette Ricardo, and Dawn Rymond is used under CC BY 4.0.
[23] Chinn et al., (2019). Development of infant reaching strategies to tactile targets on the face. Frontiers in Psychology, 10, 9. CC by 4.0
[24] Rachwani et al., (2015). The development of trunk control and its relation to reaching in infancy: A longitudinal study. Frontiers in Human Neuroscience, 9, 94. CC by 4.0
[25] Image from the CDC is in the public domain.
[26] Anekar & Bordoni (2020). Palmar grasp reflex. StatPearls. CC by 4.0
[27] Images adapted from Unsplash, Pixabay and the CDC all are in the public domain.
[28] Kaur et al., (2015). Atypical object exploration in infants at-risk for autism during the first year of life. Frontiers in Psychology, 6, 798. CC by 4.0
[29] Assortment of wooden objects by Todd LaMarr is licensed under CC by 4.0
[30] Various manipulative objects by Todd LaMarr is licensed under CC by 4.0