
4.2: Prevention and Promotion
- Last updated
- Save as PDF
- Page ID
- 46447
")
- Leonard A. Jason, Olya Glantsman, Jack F. O'Brien, and Kaitlyn N. Ramian (Editors)
- DePaul University via Rebus
Chapter Twelve Objectives
By the end of this chapter, you will be able to:
- Understand historical perspectives on prevention and promotion
- Define the different types of prevention
- Identify examples of risk and protective factors
- Describe various aspects of prevention programs and evaluation

One notable characteristic in the field of Community Psychology is the focus on prevention of problems and wellness promotion, as discussed in Chapter 1 (Jason, Glantsman, O’Brien, & Ramian, 2019). This occurs through addressing individual-level competencies within a community and also through working to change systems and contexts. As highlighted in Chapter 1, prevention serves as an exemplary framework for Community Psychology research and also an innovative way to approach real-world problems. The core belief is that taking action early on can prevent more serious problems from developing in the future. Case Study 12.1 profiles Head Start, an early childhood prevention program for kids aimed to reduce the negative effects of poverty. The case study highlights the way the political and social forces of the time shaped the development of Head Start. This program represents a pivotal tale in the history of prevention, serving as an example of many of the key concepts detailed throughout this chapter.
Case Study 12.1
The Head Start Model

Head Start, an early childhood education program for children experiencing poverty and related stressors, was first established in 1965. Head Start was created in response to President Lyndon B. Johnson’s famous State of the Union address in 1964 where he called for an “unconditional war on poverty” (Watch the speech here). Programs from this era reflected efforts to improve social conditions and prevent the negative outcomes associated with poverty.
The purpose of Head Start programming is to reduce gaps in skills, appearing at kindergarten entry, between children experiencing poverty and their counterparts. These early disparities can continue throughout schooling and into adulthood; therefore, Head Start aims to provide equitable preschool services to improve children’s readiness for entering school. The Head Start model adopts an ecological, whole-child approach and provides comprehensive services to children while promoting the well-being of the whole family that extends beyond academics (watch The Head Start Advantage for a closer look). Head Start involvement has resulted in improved language development, learning/pre-academics, and social-emotional skills of children by the time of kindergarten entry (U.S. Department of Health and Human Services Administration for Children and Families, 2010).
Since its inception over 50 years ago, Head Start has expanded and evolved greatly. See the Office of Head Start’s interactive and detailed timeline. Head Start (and Early Head Start) programs currently serve children from birth to 5 years of age. According to the Office of Head Start, there are Head Start programs across all 50 states and several US territories.
HISTORICAL PERSPECTIVES

The concept of prevention comes from the field of public health. This is very different from the medical model, which refers to the framework of treating social problems in the same manner that we treat illness. Community psychologists have long been critical of the medical model, given its shortcomings in locating social problems in the individual, which are often rooted in systematic inequalities. This talk describes key distinctions between the medical model and community-based advocacy to address female juvenile delinquency.
Two key aspects of a public health approach to problems include measuring the incidence and prevalence of disease. In Community Psychology, a public health approach requires that the focus is on measuring the incidence or prevalence of a social issue. Incidence refers to the number of new cases during a specified period of time (e.g., the annual rate of new cases of depression among women, the annual rate of new individuals who experience homelessness). Prevalence is the total number of cases in a population (e.g., the total number of women in the population with depression, the total number of people in the population who are homeless in a particular country). Understanding the incidence and prevalence of a social problem is a critical first step to developing a prevention focus.

The 1960s were a critical point in time for the change in focus to prevention, rather than treatment, of individual disease (medical model). As seen in President Johnson’s speech, a focus on prevention was in the spirit of the times. During this point in history, there was a concentrated focus on social inequality and civil rights, the prevention of mental health disorders, and the establishment of innovative prevention programming in the community (e.g., Head Start). This time was not without debates about where to focus resources and how to define social problems. For example, Albee (1983) argued forcefully against the medical model for treating mental illness. That is, no mass disorder that affects large amounts of individuals (e.g., poverty, mental illness, homelessness) has ever been eradicated by providing treatment to each person affected by the problem. Nor is it feasible to train enough professionals (e.g., clinical psychologists) to end a problem (e.g., mental illness) that has roots in deeper social problems such as poverty and oppression. Prevention efforts require an ideology aligned with social change, education, and primary prevention (Albee, 1983).
The field of prevention was somewhat new to many in the field of psychology. The public was also not familiar with this idea as it represented a very different way of thinking about solving problems. As one example, at a psychological convention in 1981, Bob Felner and Leonard Jason, two community psychologists, had a most interesting conversation with Jerry Frank, who was a senior editor at Pergamon, a major book publishing company. What often occurs at these types of meetings is that publishers and authors have discussions about possible book ideas, and Felner and Jason approached Jerry with the idea of an edited book in a new field in psychology. Jerry seemed interested, and then Felner and Jason said they wanted to title the book Preventive Psychology. Jerry looked puzzled and asked them why they would want to prevent psychology. Jerry’s reaction was actually very typical of how many people reacted to this new way of thinking about social problems. Felner and Jason chuckled and said they were not trying to prevent the field of psychology, but rather wanted to provide examples of how prevention could be used to address many problems that psychologists were dealing with such as addictions and school difficulties. Jerry had not thought about this approach before, and after a long discussion, he finally understood the exciting possibilities of this field and agreed to publish the book which was titled: Preventive Psychology: Theory, Research and Practice.
TYPES OF PREVENTION

In the wake of these debates, an abundance of programming and empirical research surfaced. This included research on preventive interventions to reduce mental illness and social problems such as crime and homelessness. The findings from these studies demonstrated that taking a prevention focus is effective (e.g., see Durlak & Wells’ 1997 meta-analysis on this topic).
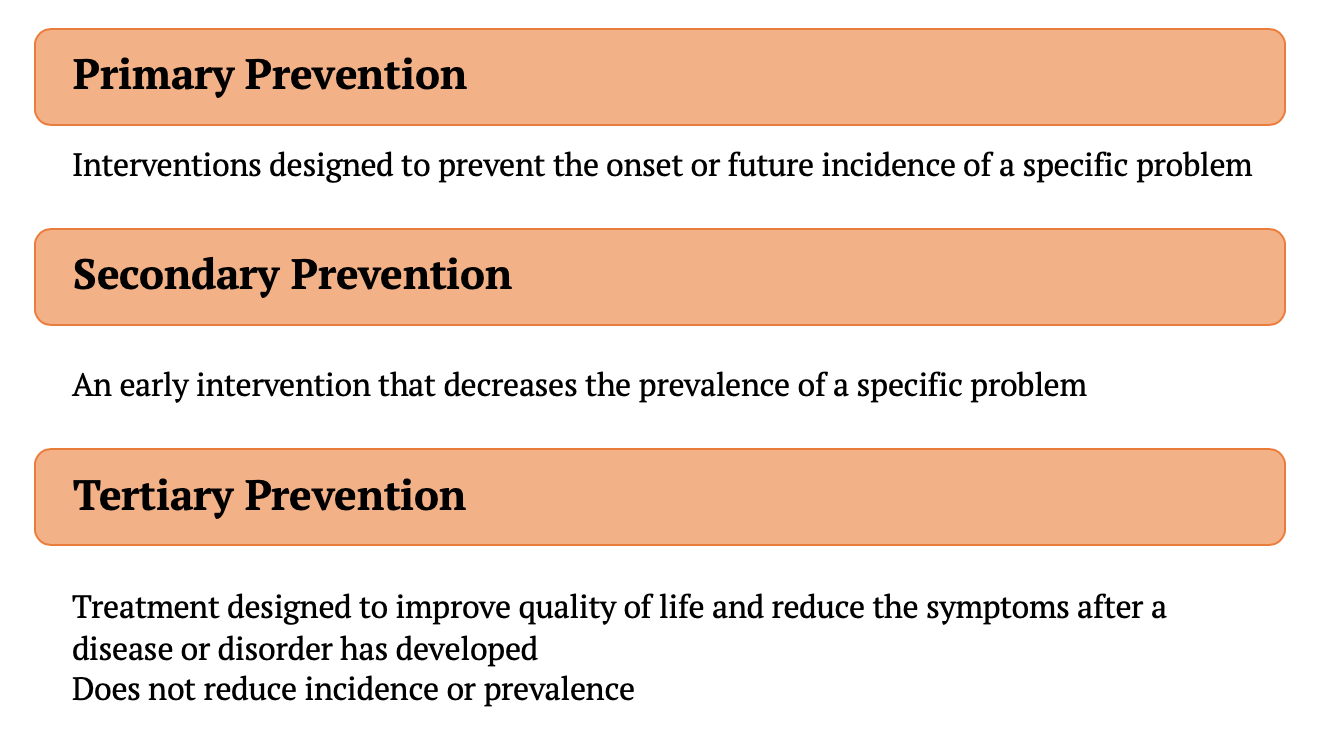
There are three types of prevention: primary, secondary, and tertiary (Caplan, 1964). The corresponding Figure 1 above provides an overview of these types of prevention. Primary prevention includes efforts to stop the problem from beginning in the first place. For example, Durlak and Wells (1997), in a meta-analysis, analyzed mental health treatment studies and outcomes from prevention interventions with another area of focus: drug use, physical health, academic achievement. They identified that specific high-quality programs can prevent multiple problems across different areas. This research specified how important it is for collaboration to occur among prevention scientists across disciplines. Collaboration and interdisciplinary work are other key focus areas of Community Psychology. Collaboration can maximize prevention efficiency and help researchers and practitioners understand the short-term and long-term effects of preventive interventions. The other important finding from this study was that positive mental health outcomes could be achieved through interventions targeting other aspects of human development and functioning. For example, (1) successful education programming can reduce future drug use and (2) programs promoting positive physical health can boost academic achievement.
Secondary prevention includes interventions that detect a disease early and prevent it from getting worse. In another meta-analysis, Durlak and Wells (1998) evaluated outcomes of 130 secondary prevention mental health programs for children and adolescents. They found that secondary prevention produces positive effects on young people receiving treatment for mental health through significantly reducing problem behavior, increasing youth competencies, and improving social and emotional adjustment. This work was groundbreaking in that it highlighted how preventive interventions can be just as effective as providing individualized psychotherapy for children and adolescents and more effective than reactive approaches to preventing problem behavior such as smoking, alcohol use, and delinquency. One case study example of secondary prevention is sexual assault prevention on college campuses. The Rape, Abuse, and Incest National Network states that college-age women have a high likelihood of experiencing sexual assault. Secondary prevention efforts to reduce sexual assault on college campuses may include self-defense, bystander intervention training, sex education regarding consent, resource education, and increasing sexual assault survivor visibility. The Centers for Disease Control and the American Psychological Association have both published recommendations to reduce sexual violence and make college campuses safer. A life transition can be stressful, such as entering school, graduating from school or getting married, and these are excellent times for implementing secondary preventive interventions. The following Case Study 12. 2 illustrates one such program from youth transferring into a new school when some children are at high risk for developing academic and social problems.
Case Study 12.2
At-Risk Youth Transferring Into a New School

A group of community psychologists designed an intervention for transferring elementary students which included an orientation to the new school and a program buddy at the new school. Also, those transferring students who were assessed as having some early academic difficulties were provided tutoring twice a week, over the entire academic year. For some at-risk youth, the tutorial aspect of the intervention focused on working directly with the children; for another group of children, the intervention focused on working with both the children and their parents. One year after the intervention ended, only children in the schools with the parental involvement condition continued to improve in their math and reading grades. The continuing increase in reading grades following the intervention suggests that students receiving both school and home tutoring benefitted the most from the comprehensive intervention. This intervention demonstrates the value of providing comprehensive prevention interventions at critical points in a child’s life course (Jason et al., 1992).
Tertiary prevention treats disease or social problems with the goal to improve quality of life and reduce symptoms of the problem after it has developed. Tertiary prevention differs from primary and secondary prevention in that it does not focus on reducing the incidence or prevalence of a disease or social problems, but rather on treating the problem once it arises. For example, as depicted in the video “An Ounce of Prevention,” parenting programs that increase key parenting characteristics, such as parental warmth, and support parents’ abilities to manage disruptive behaviors during early childhood, can prevent child maltreatment and future behavioral concerns in children. The video specifically describes the impact of such a tertiary prevention effort for a Mexican immigrant family facing several risks that may place children at greater risk for maltreatment and future behavioral distress, including underlying medical factors and poverty. These programs can be delivered to families on an individual or group basis (e.g., Incredible Years®, Triple P – Positive Parenting Program®) in the community.
The Ounce of Prevention video further depicts four prevention and promotion programs for young children, middle school adolescents, unemployed adults, and elderly people. These programs highlight each of the different types of prevention discussed above and why these programs are advantageous for their respective populations. The video includes interviews of the participants and program developers, footage of program activities, and a discussion of program outcomes. Indeed, an ounce of prevention can reduce a host of problematic behaviors and outcomes later in life.
The Institute of Medicine also has developed definitions for prevention efforts. One key distinction in this definition is that tertiary prevention is no longer considered a type of prevention, but rather an intervention strategy.
Indicated prevention refers to programming that targets people who have detectable early signs of maladjustment that foreshadow social, physical, or mental health problems. For example, the field of pediatrics has increased attention to decreasing the prevalence of childhood obesity in order to prevent adult obesity. Goldschmidt et al. (2013) specifically describe an indicated prevention approach that employed an intensive family-based treatment that included a combination of dieting, exercise, and behavioral (e.g., self-monitoring, parent skill training) strategies that targeted 669 obese and overweight youth across three cities in the US. Researchers measured the change in weight that was necessary to alter the status of overweight or obese youth to non-overweight. Results showed that despite some differences by age and initial weight classification, even a small decrease in weight was enough to move children into the non-overweight status after one year. Specifically, this underscores that preventive efforts during childhood may need only a small investment of resources to produce important changes. Another example of indicated prevention programs targeting substance use among youth can be found here.
Selective prevention involves programming that targets individuals who do not show any indication of the problem, but are at high risk for the development of the problem. For example, Head Start can be considered a type of selective prevention because many programs aim to provide comprehensive supports (e.g., schooling, family-based interventions) to children experiencing specific risk factors that place children at risk for later academic and social-emotional difficulties, such as poverty or developmental delays.
Universal prevention, which is similar to primary prevention, targets all of the people in a given population. School-based universal prevention programs that target behavioral and social-emotional functioning at the school or class-wide level are an example of a universal prevention approach to increasing access to services. These programs are a direct response to literature which indicated that the unmet behavioral and mental health needs of school-aged children increase the risk for longer-term declines in mental health, academic, and social functioning (Costello, Egger, & Angold, 2005; Nastasi, 2004). One such prevention approach to population health that has demonstrated immediate and long-term behavioral, academic, and societal benefits, the PAX Good Behavior Game, is described in Case Study 12.3.
Case Study 12.3
The PAX Good Behavior Game®

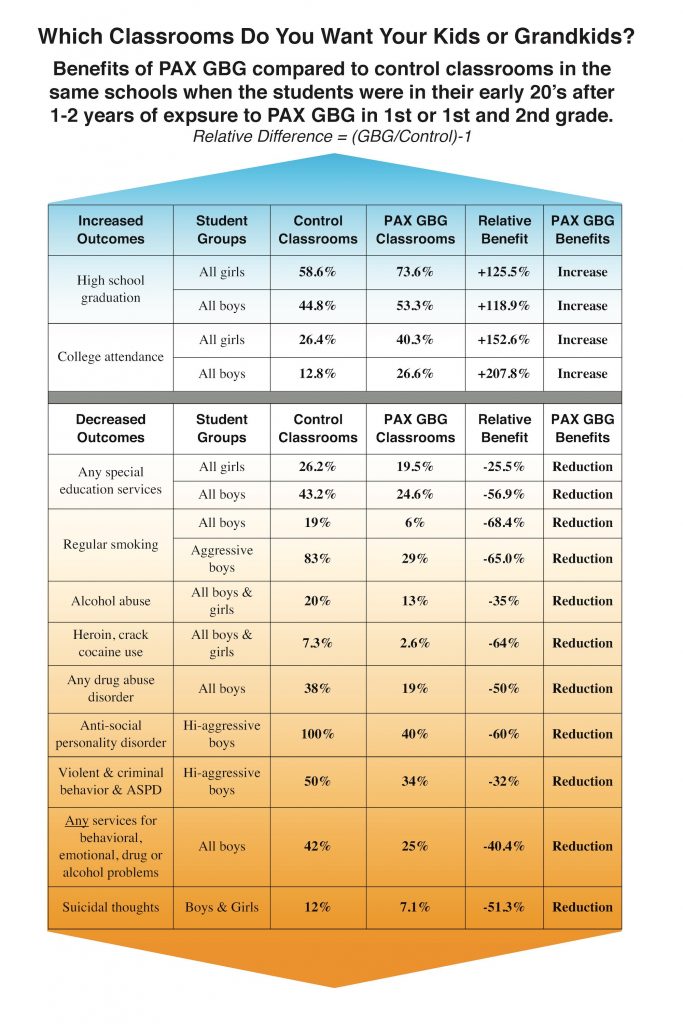
The PAX Good Behavior Game® is a set of universal prevention strategies, rooted in decades of behavioral science that are implemented by classroom teachers in schools. PAX GBG aims to create a positive, safe, and nurturing classroom environment for learning and pro-social interactions. This nurturing environment enhances children’s behavioral skills, such as self-regulation and co-regulation with other classmates, and can improve learning outcomes in children. PAX is an example of universal prevention because it targets and benefits all students in a classroom or school, including the students who are exhibiting signs of behavioral and/or learning concerns as well as those who are not exhibiting these concerns. Click here to learn more about the good behavior game and watch Dr. Dennis Embry, president and senior scientist at PAXIS Institute talk about PAX.
In addition to immediate changes in the classroom, such as fewer instances of discipline referrals, studies have shown that children who were in PAX GBG classrooms during elementary school were less likely to use tobacco and other substances and more likely to experience better behavior and mental health in high school and young adulthood (e.g., Storr, Ialongo, Kellam, & Anthony, 2002; Wilcox et al., 2008). Learn more about some of the short and long-term benefits of PAX GBG here.
* PAX Good Behavior Game images reproduced with permission from PAXIS Institute
PROMOTION

Related to the key concept of primary prevention is promotion. Promotion involves empowering individuals to increase control of their health and well-being through literacy and programming. Community psychologists identified that the goal of preventing problems can be done through promoting well-being. Generally, there are two approaches to promotion. The first is through reducing the chances that the problem will arise. The second is through increasing skills, strengths, and competencies of individuals and settings to reduce the risk for problems arising. Cost-benefit analyses of promotion have shown that efforts that focus on health promotion are very cost-effective compared to reactive or treatment-oriented approaches (Durlak & Wells, 1997). Community psychologists argue that promotion must also take into consideration ecological approaches to improving the human condition. That is, those who are interested in preventing social problems and promoting human competencies and well-being must call attention to the relationship between broader social forces and rates of disease and social distress seen in communities (Albee, 1983). For example, Case Study 12.4 describes a community-based advocacy program developed by community psychologists to promote well-being among girls in the juvenile justice system.
Case Study 12.4
Resilience, Opportunity, Safety, Education, Strength (ROSES)

Resilience, Opportunity, Safety, Education, Strength is a community-based program in New York City that pairs a trained advocate with girls involved with or at-risk for juvenile justice system involvement. The program works to provide the girls with resources and education, defining personal goals, developing self-efficacy skills, encouraging engagement with various social contexts (i.e., school, family, peers) and promotion to reduce justice system involvement. Resilience, Opportunity, Safety, Education, Strength aims to learn more about justice-system-involved girls’ needs. Research shows that those girls who have participated in this program reported greater resilience and self-efficacy; fewer risk behaviors, including violence, crime, and substance use; and decreased negative emotions such as depression, anxiety, and anger (Javdani & Allen, 2016).
Learn more about ROSES.
Risk and Protective Factors

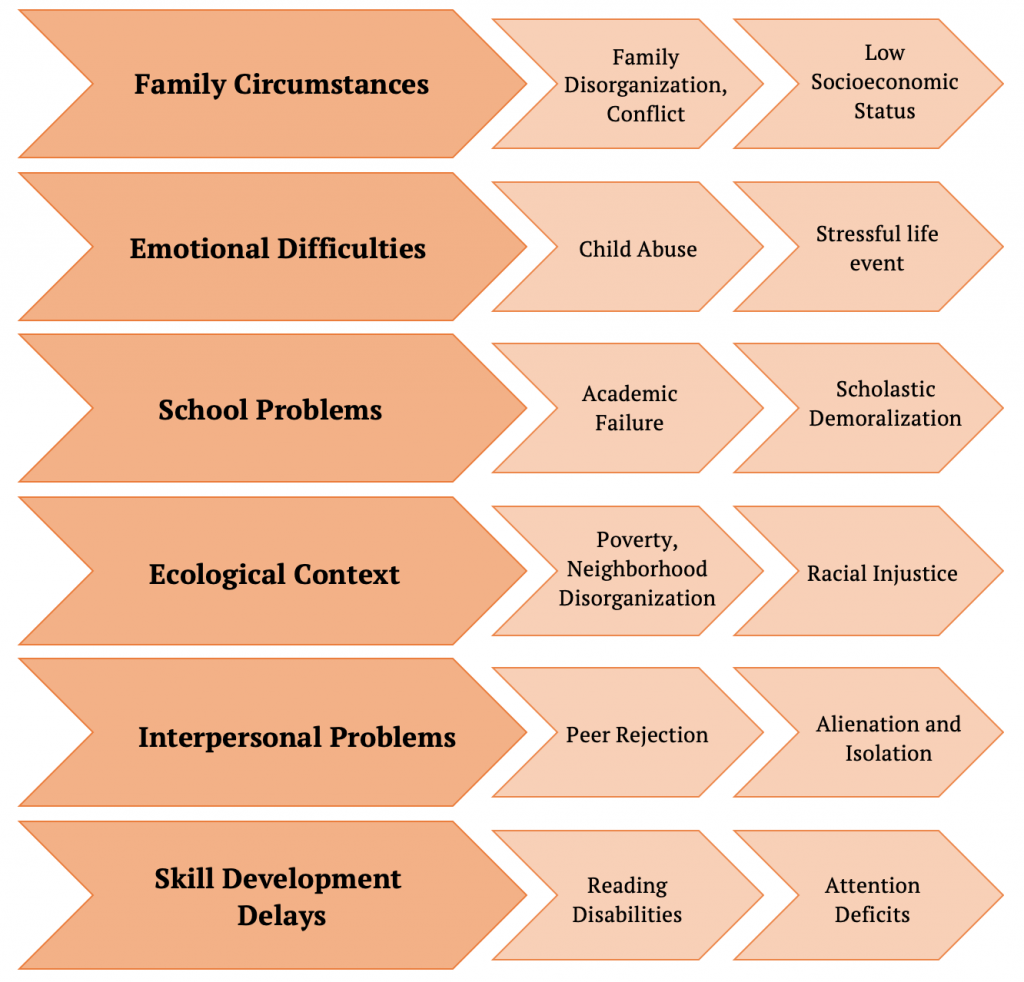
Another key concept is the role of risk and protective factors. Risk factors are variables that are related to an increased risk for developing a disease or problem. While the term comes from a public health perspective, community psychologists use risk factors to understand factors associated with increased risk for various social problems such as homelessness, juvenile delinquency, or gender-based violence. For example, Figure 3 below depicts some of the most common risk factors, especially among children and adolescents, which prevention programs need to consider in reducing the development of social problems. Case Study 12.5 provides a specific example of risk factors for human trafficking, a pervasive problem around the globe. In contrast to risk factors, protective factors include variables that are related to a decreased risk for developing a disease or a social problem. Protective factors can include variables such as positive relationships, academic achievement, parental support, and strong economic conditions.
Case Study 12.5
The Most Vulnerable, The Risk Factors, and The Most Effective Programming

Human trafficking is a serious social problem in the US and around the world. Human trafficking involves the use of force, fraud, or coercion for commercial sex or involuntary labor (Trafficking Victims Protection Act of 2000). For sex trafficking cases, there are a number of risk factors for youth. Taking an ecological perspective, these can include factors related to an individual’s sociodemographic characteristics as well as social, behavioral, and broader community risk factors. Figure 4 below includes a list of risk factors for human trafficking.
Thus, the most effective prevention programming, such as The Prevention Project program, should target the most vulnerable population (e.g., female youth) engaged in social or behavioral correlates of sex trafficking (e.g., running away), or involved with community systems and programs such as the juvenile justice system or foster care, or social problems more generally, like poverty. The most effective types of services tend to be integrated and target multiple risk factors.

PREVENTION RESEARCH AND PROGRAMMING

The Institute of Medicine (1994) developed a model for problem assessment, intervention, and dissemination strategies. For example, this research cycle includes assessing the prevalence of risk and protective factors of a problem area, developing prevention innovations, researching the effectiveness of those innovations, and disseminating innovations into the community. Figure 5 below outlines each aspect of the preventive intervention research cycle.
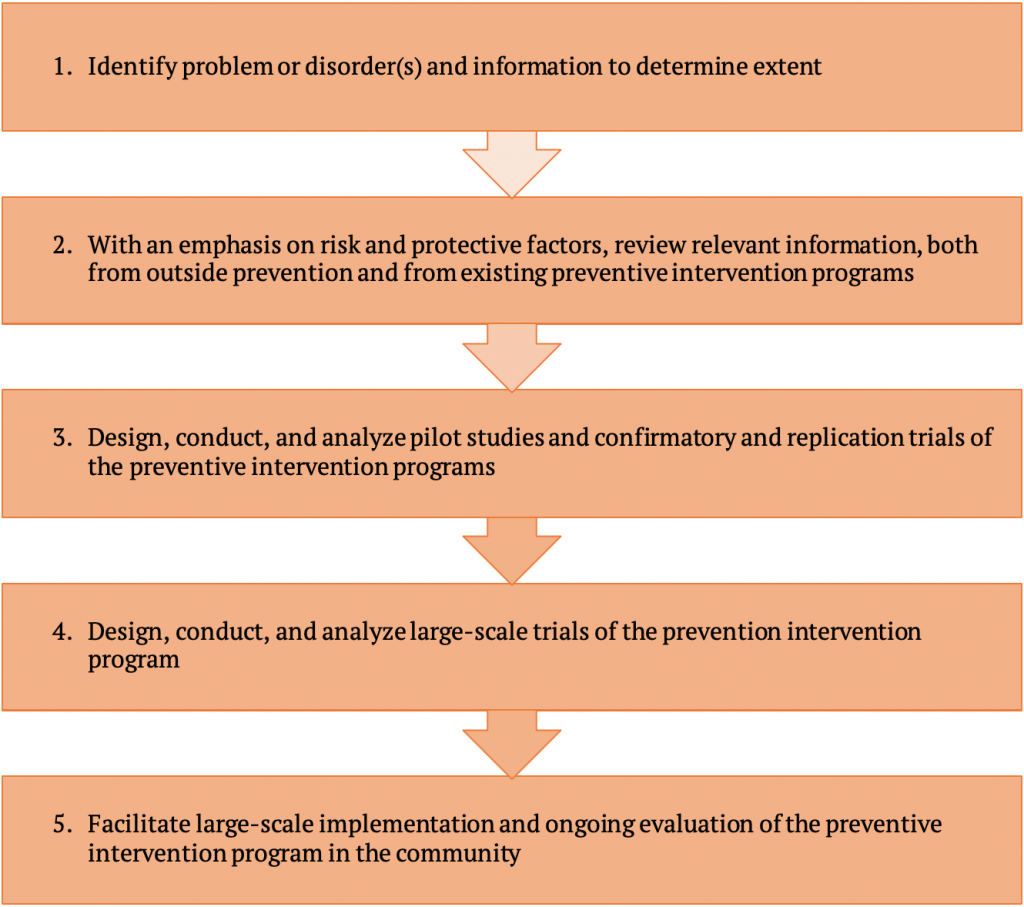
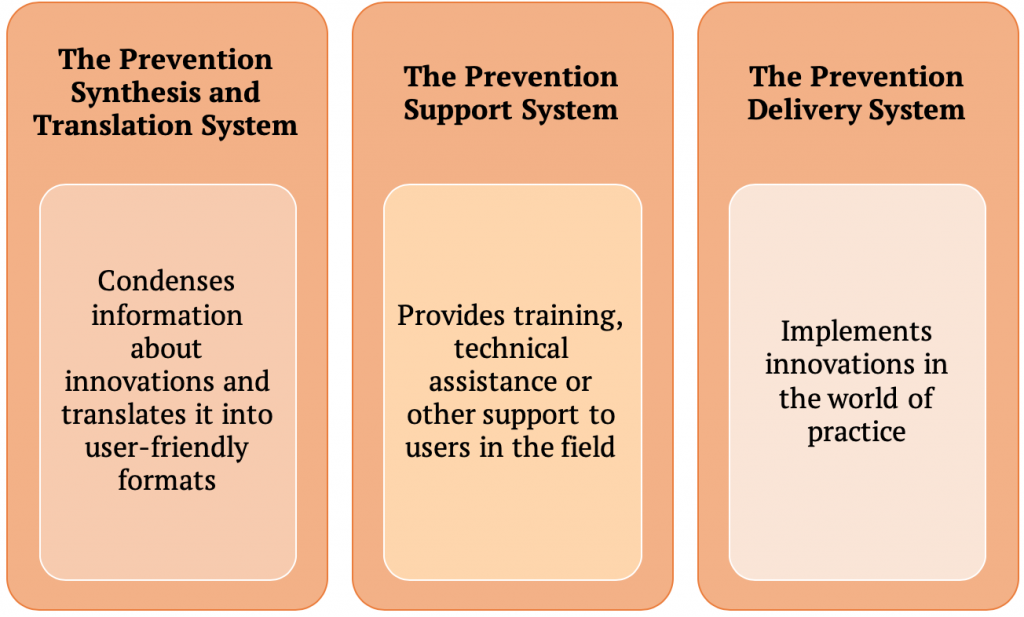
There are a number of challenges to conducting prevention research and using these models since they identify what needs to be done but provide very little detail on how these things will happen. Most models, such as the Institute of Medicine framework, focus on the functions that are part of the innovation, implementation, and dissemination process, but not on the systems that support these functions. To address this gap, Wandersman and colleagues (2008) proposed a framework that describes relevant systems to help bridge the gap. The Interactive Systems Framework works to connect step four (conducting trials of the program) and step five (implementing the program in the community) of the Institute of Medicine model. Figure 6 below details the critical components of the Interactive Systems Framework to bridge this gap. For example, Halgunseth and colleagues (2012) used the Interactive Systems Framework to understand the relationship between program capacity and implementation in after-school settings. They examined eight after-school sites that received the Good Behavior Game (described in Case Study 12.2). Aligned with the Prevention Support System element of the Interactive Systems Framework, the after-school staff was trained and received weekly on-site support in implementing the intervention. It was found that after-school settings that were more organized and maintained strong links to individuals or community-based organizations scored higher in program fidelity and quality. Funders can utilize the Interactive Systems Framework to identify what kinds of support they should provide for the Prevention Synthesis and Translation System element; similarly, practitioners can gather information from that same component for what they need as well as from the Prevention Support System element. Additionally, practitioners can see what they need to do to build capacity from the perspective of the Prevention Delivery System component.
Program evaluation is a cornerstone of Community Psychology research and action. Broadly, program evaluation involves measuring the effectiveness of interventions and policies. This can include both processes (e.g., how were intervention activities implemented) and outcomes (e.g., did the intervention achieve the outcome objectives). Community psychologists engaged in prevention and promotion research and action use logic models to guide these efforts. To read more about program evaluation, check out these resources from the Centers for Disease Control and the Community Tool Box. Conducting program evaluations is a key way that community psychologists can measure whether or not our prevention and promotion efforts are having the intended effect.
CRITIQUES OF THE PREVENTION PARADIGM

Even though prevention and promotion are seminal concepts in Community Psychology, they are not without drawbacks. Community psychologists have outlined two key critiques. First, prevention and promotion is limited in its focus on empowerment (Rappaport, 1981). Rappaport argued that prevention is “one-sided” in part because it is derived from a needs model, rather than a rights model. Further, Rappaport argued prevention programs may not be enough to change social institutions, but rather just add on to what is already in place. Rappaport made the case that empowerment is a better model because it prioritizes rights and offers a more transformative perspective to change social problems. Second, Miller and Shinn (2005) outlined another critique of prevention and promotion: the failure to adopt prevention programming is rooted in difficulties in implementation and dissemination.
Miller and Shinn (2005) described potential problems with the Institute of Medicine model of dissemination and potential ways community psychologists can directly counteract these problems in their dissemination efforts. They identified four distinct problems in disseminating prevention and promotion innovations. First, many communities have limited capacity (as shown in the video link) to implement a program causing dissemination failure. The context in which community-based organizations function shapes that capacity, so folks interested in disseminating programs must take into account ecological factors. Second, often times there is an incongruence of values—a lack of compatibility and/or consistency between the setting and the prevention program. Third, Miller and Shinn argued that there is a presumption that innovations that “prove their worth” in a controlled, experimental setting are better than what they might replace when implemented. They referred to this as “innovation bias” that wrongly characterizes communities as passively waiting to adopt a prevention program rather than problem-solving themselves. Finally, they argued that the Institute of Medicine prevention and promotion model proposes an overly simplistic model of decision-making. It assumes that the evidence of the success of an innovation in a controlled, experimental setting is sufficient to promote decisions about adopting the innovation in practice. We know that many other considerations are also relevant in the decision-making of community agencies. Miller and Shinn (2005) proposed two potential solutions to these pitfalls of the Institute of Medicine framework. Rather than curating innovations in the context of a university and then translating them to a different environment in the community, community psychologists should identify promising prevention and promotion interventions already functioning in communities and study those to understand their effectiveness. Finally, they proposed that researchers should focus less on specific programs and more on powerful ideas that can improve the quality of life. This focus on powerful ideas may actually come from the process of understanding how prevention and promotion programs work in communities by specifying the core elements of a program that could be applied in other community contexts. Thus, we should be “learning from communities” and disseminating their prevention and promotion efforts that work.
Despite these critiques, prevention is still an important framework in Community Psychology and has the potential to create sustainable change in communities. Looking at precipitating factors, an attempt is made to make meaningful changes in environmental or personal factors to eliminate the barriers to success and wellness. Disease and community disorder will always require reactive responses and treatment; however, one goal of Community Psychology is to prevent some of it. Prevention lowers the demand for treatment and allows for increased access to resources that individuals may otherwise not have access to. As noted in this chapter, prevention also has the potential to reduce societal costs in the long run, which means resources can continue being spread for a greater amount of time.
SUMMING UP

This chapter outlined the importance of prevention and promotion as key concepts in Community Psychology. We highlighted the historical and contemporary perspectives on prevention and promotion including different types of prevention (e.g., primary, secondary, tertiary), risk and protective factors, and the various aspects of prevention programs and the techniques needed to evaluate such programming. As seen throughout the chapter based on the wide range of examples—from childhood obesity prevention efforts to examining risk factors for human trafficking—there are a vast number of social issues community psychologists can explore with an eye towards prevention and promotion. These are important frameworks to use to target change across multiple levels (e.g., individuals, groups, settings, social systems) in order to prevent negative outcomes and promote well-being.
Critical Thought Questions
- What role do risk factors play in promotion? Why is that important?
- How have historical debates on prevention and promotion shaped the way we view their usefulness currently?
- How does each type of prevention impact problems experienced in society or by members of society?
- What aspects must we consider regarding prevention research and programming?
Take the Chapter 12 Quiz
View the Chapter 12 Lecture Slides
____________________________________________________________________
REFERENCES
Albee, G. W. (1983). Preventing psychopathology and promoting human potential. American Psychologist, 37, 1043–1050.
Caplan, G. (1964). Principles of Preventive Psychiatry. New York, NY: Basic Books.
Costello, E. J., Egger, H., & Angold, A. (2005). 10-year research update review: the epidemiology of child and adolescent psychiatric disorders: I. Methods and public health burden. Journal of the American Academy of Child & Adolescent Psychiatry, 44(10), 972-986.
Durlak, J. A., & Wells, A. M. (1997). Primary prevention mental health programs for children and adolescents: a meta-analytic review. American Journal of Community Psychology, 25, 115-152.
Durlak, J. A. & Wells, A. M. (1998). Evaluation of indicated preventative intervention (secondary prevention) mental health programs for children and adolescents. American Journal of Community Psychology, 26, 775-802.
Goldschmidt, A. B., Wilfley, D. E., Paluch, R. A., Roemmich, J. N., & Epstein, L. H. (2013). Indicated prevention of adult obesity: How much weight change is necessary for normalization of weight status in children?. JAMA Pediatrics, 167(1), 21-26.
Halgunseth, L. C., Carmack, C., Childs, S. S., Caldwell, L., Craig, A., & Smith, E. P. (2012). Using the Interactive Systems Framework in understanding the relation between program capacity and implementation in afterschool settings. American Journal of Community Psychology, 50, 311-320.
Jason, L. A., Glantsman, O., O’Brien, J. F., & Ramian, K. N. (2019). Introduction to the field of Community Psychology. In L. A. Jason, O Glantsman, J. F. O’Brien, & K. N. Ramian (Eds.), Introduction to Community Psychology: Becoming an agent of change. Retrieved from https://press.rebus.community/introductiontocommunitypsychology/chapter/intro-to-community-psychology/
Jason, L. A., Weine, A. W., Johnson, J. H., Warren-Sohlberg, L, Filippelli, L. A., Turner, E. Y., & Lardon, C. (1992). Helping Transfer Students. San Francisco, CA: Jossey-Bass.
Javdani, S., & Allen, N. E. (2016). An ecological model for intervention for juvenile justice-involved girls: Development and preliminary prospective evaluation. Feminist Criminology, 11(2), 135-162.
Miller, R. L. & Shinn, M. (2005). Learning from communities: Overcoming difficulties in dissemination of prevention and promotion efforts. American Journal of Community Psychology, 35(3-4), 169-183.
Mrazek, P. J., Haggerty, R. J., & The Institute of Medicine, Committee on Prevention of Mental Disorders, Division of Biobehavorial Sciences and Mental Disorders. (1994). Reducing risks for mental disorders: Frontiers for preventive intervention research. Washington, DC: National Academy Press.
Nastasi, B. K. (2004). Meeting the challenges of the future: Integrating public health and public education for mental health promotion. Journal of Educational and Psychological Consultation, 15(3-4), 295-312.
Rappaport, J. (1981). In praise of paradox: A social policy of empowerment over prevention. American Journal of Community Psychology, 9(1), 1.
Storr, C. L., Ialongo, N. S., Kellam, S. G., & Anthony, J. C. (2002). A randomized controlled trial of two primary school intervention strategies to prevent early onset tobacco smoking. Drug and Alcohol Dependence, 66(1), 51-60.
U.S. Department of Health and Human Services Administration for Children and Families. (2010). Directory of program services. Washington, DC. Office of Public Affairs. Retrieved from http://www.ncdsv.org/images/ACF_DirectoryOfProgramServices.pdf
Trafficking Victims Protection Act of 2000. 22 U.S.C § 7101.
Wandersman, A., Duffy, J., Flaspholer, P., Noonan, R., Lubell, K., Stillman, L., … Saul, J. (2008). Bridging the gap between prevention research and practice: The interactive systems framework for dissemination and implementation. American Journal of Community Psychology, 41, 171-181.
Wilcox, H. C., Kellam, S. G., Brown, C. H., Poduska, J. M., Ialongo, N. S., Wang, W., & Anthony, J. C. (2008). The impact of two universal randomized first-and second-grade classroom interventions on young adult suicide ideation and attempts. Drug and Alcohol Dependence, 95, S60-S73.
