
13.2: Decision Making
- Last updated
- Save as PDF
- Page ID
- 91984

- Wikipedia
According to the different levels of consequences, each process of making a decision requires appropriate effort and various aspects to be considered. The following excerpt from the story about Knut makes this obvious: “After considering facts like the warm weather in Spain and shirts and shorts being much more comfortable in this case (information gathering and likelihood estimation) Knut reasons that he needs them for his vacation. In consequence, he finally makes the decision to pack mainly shirts and shorts in his bag (final act of choosing).” Now it seems like there cannot be any decision making without previous reasoning, but that is not true. Of course there are situations in which someone decides to do something spontaneously, with no time to reason about it. We will not go into detail here but you might think about questions like "Why do we choose one or another option in that case?"
Choosing among alternatives
The psychological process of decision making constantly goes along with situations in daily life. Thinking about Knut again we can imagine him to decide between packing more blue or more green shirts for his vacation (which would only have minor consequences) but also about applying a specific job or having children with his wife (which would have relevant influence on important circumstances of his future life). The mentioned examples are both characterized by personal decisions, whereas professional decisions, dealing for example with economic or political issues, are just as important.
The utility approach
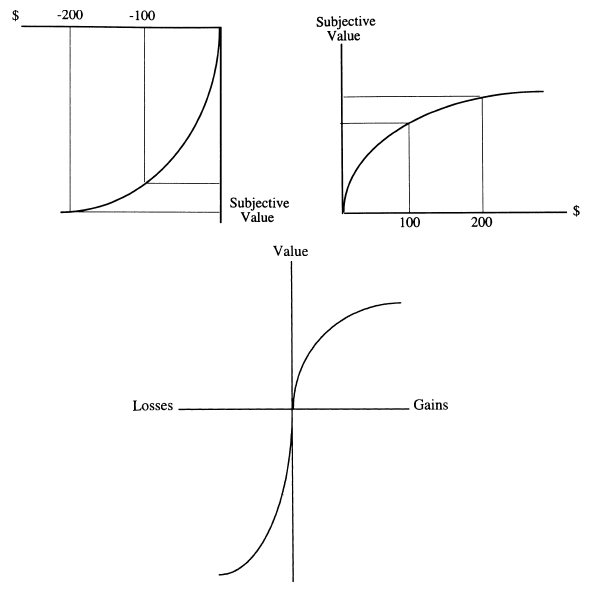
Figure 6, Relation between (monetary) gains/losses and their subjective value according to Prospect Theory
There are three different ways to analyze decision making. The normative approach assumes a rational decision-maker with well-defined preferences. While the rational choice theory is based on a priori considerations, the descriptive approach is based on empirical observations and on experimental studies of choice behavior. The prescriptive enterprise develops methods in order to improve decision making. According to Manktelow and Reber´s definition, “utility refers to outcomes that are desirable because they are in the person’s best interest” (Reber, A. S., 1995; Manktelow, K., 1999). This normative/descriptive approach characterizes optimal decision making by the maximum expected utility in terms of monetary value. This approach can be helpful in gambling theories, but simultaneously includes several disadvantages. People do not necessarily focus on the monetary payoff, since they find value in things other than money, such as fun, free time, family, health and others. But that is not a big problem, because it is possible to apply the graph (Figure 6), which shows the relation between (monetary) gains/losses and their subjective value / utility, which is equal to all the valuable things mentioned above. Therefore, not choosing the maximal monetary value does not automatically describe an irrational decision process.
Misleading effects
But even respecting the considerations above there might still be problems to make the “right” decision because of different misleading effects, which mainly arise because of the constraints of inductive reasoning. In general this means that our model of a situation/problem might not be ideal to solve it in an optimal way. The following three points are typical examples for such effects.
Subjective models
This effect is rather equal to the illusory correlations mentioned before in the part about the constraints of inductive reasoning. It is about the problem that models which people create might be misleading, since they rely on subjective speculations. An example could be deciding where to move by considering typical prejudices of the countries (e.g. always good pizza, nice weather and a relaxed life-style in Italy in contrast to some kind of boring food and steady rain in Great Britain). The predicted events are not equal to the events occurring indeed. (Kahneman & Tversky, 1982; Dunning & Parpal, 1989)
Focusing illusion
Another misleading effect is the so-called focusing illusion. By considering only the most obvious aspects in order to make a certain decision (e.g. the weather) people often neglect various really important outcomes (e.g. circumstances at work). This effect occurs more often, if people judge about others compared with judgments about their own living.
Framing effect
A problem can be described in different ways and therefore evoke different decision strategies. If a problem is specified in terms of gains, people tend to use a risk-aversion strategy, while a problem description in terms of losses leads to apply a risk-taking strategy. An example of the same problem and predictably different choices is the following experiment: A group of people is asked to imagine themselves $300 richer than they are, is confronted with the choice of a sure gain of $100 or an equal chance to gain $200 or nothing. Most people avoid the risk and take the sure gain, which means they take the risk-aversion strategy. Alternatively if people are asked to assume themselves to be $500 richer than in reality, given the options of a sure loss of $100 or an equal chance to lose $200 or nothing, the majority opts for the risk of losing $200 by taking the risk seeking or risk-taking strategy. This phenomenon is known as framing effect and can also be illustrated by Figure 6 above, which is a concave function for gains and a convex one for losses. (Foundations of Cognitive Psychology, Levitin, D. J., 2002)
Justification in decision making
Decision making often includes the need to assign a reason for the decision and therefore justify it. This factor is illustrated by an experiment by A. Tversky and E. Shafir (1992): A very attractive vacation package has been offered to a group of students who have just passed an exam and to another group of students who have just failed the exam and have the chance to rewrite it after the holidays coming up. All students have the options to buy the ticket straight away, to stay at home, or to pay $5 for keeping the option open to buy it later. At this point, there is no difference between the two groups, since the number of students who passed the exam and decided to book the flight (with the justification of a deserving a reward), is the same as the number of students who failed and booked the flight (justified as consolation and having time for reoccupation). A third group of students who were informed to receive their results in two more days was confronted with the same problem. The majority decided to pay $5 and keep the option open until they would get their results. The conclusion now is that even though the actual exam result does not influence the decision, it is required in order to provide a rationale.
Executive functions
Figure 7, Left frontal lobe
Subsequently, the question arises how this cognitive ability of making decisions is realized in the human brain. As we already know that there are a couple of different tasks involved in the whole process, there has to be something that coordinates and controls those brain activities – namely the executive functions. They are the brain's conductor, instructing other brain regions to perform, or be silenced, and generally coordinating their synchronized activity (Goldberg, 2001). Thus, they are responsible for optimizing the performance of all “multi-threaded” cognitive tasks.
Locating those executive functions is rather difficult, as they cannot be appointed to a single brain region. Traditionally, they have been equated with the frontal lobes, or rather the prefrontal regions of the frontal lobes; but it is still an open question whether all of their aspects can be associated with these regions.
Nevertheless, we will concentrate on the prefrontal regions of the frontal lobes, to get an impression of the important role of the executive functions within cognition. Moreover, it is possible to subdivide these regions into functional parts. But it is to be noted that not all researchers regard the prefrontal cortex as containing functionally different regions.
Executive functions in practice
According to Norman and Shallice, there are five types of situations in which executive functions may be needed in order to optimize performance, as the automatic activation of behaviour would be insufficient. These are situations involving...
1. ...planning or decision making.
2. ...error correction or trouble shooting.
3. ...responses containing novel sequences of actions.
4. ...technical difficulties or dangerous circumstances.
5. ...the control of action or the overcoming of strong habitual responses.
The following parts will have a closer look to each of these points, mainly referring to brain-damaged individuals.
Surprisingly, intelligence in general is not affected in cases of frontal lobe injuries (Warrington, James & Maciejewski, 1986). However, dividing intelligence into crystallised intelligence (based on previously acquired knowledge) and fluid intelligence (meant to rely on the current ability of solving problems), emphasizes the executive power of the frontal lobes, as patients with lesions in these regions performed significantly worse in tests of fluid intelligence (Duncan, Burgess & Emslie, 1995).
1. Planning or decision making
Impairments in abstract and conceptual thinking
To solve many tasks it is important that one is able to use given information. In many cases, this means that material has to be processed in an abstract rather than in a concrete manner. Patients with executive dysfunction have abstraction difficulties. This is proven by a card sorting experiment (Delis et al., 1992):
The cards show names of animals and black or white triangles placed above or below the word. Again, the cards can be sorted with attention to different attributes of the animals (living on land or in water, domestic or dangerous, large or small) or the triangles (black or white, above or below word). People with frontal lobe damage fail to solve the task because they cannot even conceptualize the properties of the animals or the triangles, thus are not able to deduce a sorting-rule for the cards (in contrast, there are some individuals only perseverating; they find a sorting-criterion, but are unable to switch to a new one).
These problems might be due to a general difficulty in strategy formation.
Goal directed behavior
Let us again take Knut into account to get an insight into the field of goal directed behaviour – in principle, this is nothing but problem solving since it is about organizing behavior towards a goal. Thus, when Knut is packing his bag for his holiday, he obviously has a goal in mind (in other words: He wants to solve a problem) – namely get ready before the plane starts. There are several steps necessary during the process of reaching a certain goal:
Goal must be kept in mind
Knut should never forget that he has to pack his bag in time.
Dividing into subtasks and sequencing
Knut packs his bag in a structured way. He starts packing the crucial things and then goes on with rest.
Completed portions must be kept in mind
If Knut already packed enough underwear into his bag, he would not need to search for more.
Flexibility and adaptability
Imagine that Knut wants to pack his favourite T-Shirt, but he realizes that it is dirty. In this case, Knut has to adapt to this situation and has to pick another T-Shirt that was not in his plan originally.
Evaluation of actions
Along the way of reaching his ultimate goal Knut constantly has to evaluate his performance in terms of ‘How am I doing considering that I have the goal of packing my bag?’.
Executive dysfunction and goal directed behavior
The breakdown of executive functions impairs goal directed behavior to a large extend. In which way cannot be stated in general, it depends on the specific brain regions that are damaged. So it is quite possible that an individual with a particular lesion has problems with two or three of the five points described above and performs within average regions when the other abilities are tested. However, if only one link is missing from the chain, the whole plan might get very hard or even impossible to master. Furthermore, the particular hemisphere affected plays a role as well.
Another interesting result was the fact that lesions in the frontal lobes of left and right hemisphere impaired different abilities. While a lesion in the right hemisphere caused trouble in making recency judgements, a lesion in the left hemisphere impaired the patient’s performance only when the presented material was verbal or in a variation of the experiment that required self-ordered sequencing. Because of that we know that the ability to sequence behaviour is not only located in the frontal lobe but in the left hemisphere particularly when it comes to motor action.
Problems in sequencing
In an experiment by Milner (1982), people were shown a sequence of cards with pictures. The experiment included two different tasks: recognition trials and recency trials. In the former the patients were shown two different pictures, one of them has appeared in the sequence before, and the participants had to decide which one it was. In the latter they were shown two different pictures, both of them have appeared before, they had to name the picture that was shown more recently than the other one. The results of this experiment showed that people with lesions in temporal regions have more trouble with the recognition trial and patients with frontal lesions have difficulties with the recency trial since anterior regions are important for sequencing. This is due to the fact that the recognition trial demanded a properly functioning recognition memory, the recency trial a properly functioning memory for item order. These two are dissociable and seem to be processed in different areas of the brain.
The frontal lobe is not only important for sequencing but also thought to play a major role for working memory. This idea is supported by the fact that lesions in the lateral regions of the frontal lobe are much more likely to impair the ability of 'keeping things in mind' than damage to other areas of the frontal cortex do.
But this is not the only thing there is to sequencing. For reaching a goal in the best possible way it is important that a person is able to figure out which sequence of actions, which strategy, best suits the purpose, in addition to just being able to develop a correct sequence. This is proven by an experiment called 'Tower of London' (Shallice, 1982) which is similar to the famous 'Tower of Hanoi' task with the difference that this task required three balls to be put onto three poles of different length so that one pole could hold three balls, the second one two and the third one only one ball, in a way that a changeable goal position is attained out of a fixed initial position in as few moves as possible. Especially patients with damage to the left frontal lobe proved to work inefficiently and ineffectively on this task. They needed many moves and engaged in actions that did not lead toward the goal.
Problems with the interpretation of available information
Quite often, if we want to reach a goal, we get hints on how to do it best. This means we have to be able to interpret the available information in terms of what the appropriate strategy would be. For many patients of executive dysfunction this is not an easy thing to do either. They have trouble to use this information and engage in inefficient actions. Thus, it will take them much longer to solve a task than healthy people who use the extra information and develop an effective strategy.
Problems with self-criticism and -monitoring
The last problem for people with frontal lobe damage we want to present here is the last point in the above list of properties important for proper goal directed behavior. It is the ability to evaluate one's actions, an ability that is missing in most patients. These people are therefore very likely to 'wander off task' and engage in behavior that does not help them to attain their goal. In addition to that, they are also not able to determine whether their task is already completed at all. Reasons for this are thought to be a lack of motivation or lack of concern about one's performance (frontal lobe damage is usually accompanied by changes in emotional processing) but these are probably not the only explanations for these problems.
Another important brain region in this context – the medial portion of the frontal lobe – is responsible for detecting behavioral errors made while working towards a goal. This has been shown by ERP experiments where there was an error-related negativity 100ms after an error has been made. If this area is damaged, this mechanism cannot work properly any more and the patient loses the ability to detect errors and thus monitor his own behavior.
However, in the end we must add that although executive dysfunction causes an enormous number of problems in behaving correctly towards a goal, most patients when assigned with a task are indeed anxious to solve it but are just unable to do so.
2. Error correction and trouble shooting
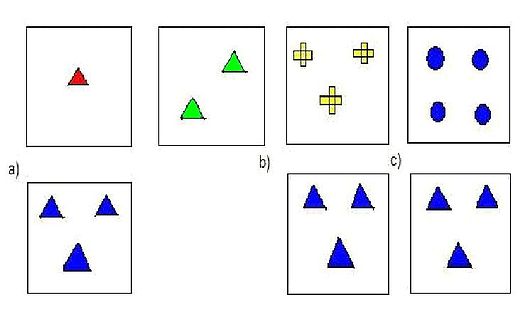
Figure 8, Example for the WCST: Cards sorted according to shape (a), number (b) or color (c) of the objects
The most famous experiment to investigate error correction and trouble shooting is the Wisconsin Card Sorting Test (WCST). A participant is presented with cards that show certain objects. These cards are defined by shape, color and number of the objects on the cards. These cards now have to be sorted according to a rule based on one of these three criteria. The participant does not know which rule is the right one but has to reach the conclusion after positive or negative feedback of the experimenter. Then at some point, after the participant has found the correct rule to sort the cards, the experimenter changes the rule and the previous correct sorting will lead to negative feedback. The participant has to realize the change and adapt to it by sorting the cards according to the new rule.
Patients with executive dysfunction have problems identifying the rule in the first place. It takes them noticeably longer because they have trouble using already given information to make a conclusion. But once they got to sorting correctly and the rule changes, they keep sorting the cards according to the old rule although many of them notice the negative feedback. They are just not able to switch to another sorting-principle, or at least they need many tries to learn the new one. They perseverate.
Problems in shifting and modifying strategies
Intact neuronal tissue in the frontal lobe is also crucial for another executive function connected with goal directed behavior that we described above: Flexibility and adaptability. This means that persons with frontal lobe damage will have difficulties in shifting their way of thinking – meaning creating a new plan after recognizing that the original one cannot be carried out for some reason. Thus, they are not able to modify their strategy according to this new problem. Even when it is clear that one hypothesis cannot be the right one to solve a task, patients will stick to it nevertheless and are unable to abandon it (called 'tunnel vision').
Moreover, such persons do not use as many appropriate hypotheses for creating a strategy as people with damage to other brain regions do. In what particular way this can be observed in patients can again not be stated in general but depends on the nature of the shift that has to be made.
These earlier described problems of 'redirecting' of one's strategies stand in contrast to the actual 'act of switching' between tasks. This is yet another problem for patients with frontal lobe damage. Since the control system that leads task switching as such is independent from the parts that actually perform these tasks, the task switching is particularly impaired in patients with lesions to the dorsolateral prefrontal cortex while at the same time they have no trouble with performing the single tasks alone. This of course, causes a lot of problems in goal directed behavior because as it was said before: Most tasks consist of smaller subtasks that have to be completed.
3. Responses containing novel sequences of actions
Many clinical tests have been done, requiring patients to develop strategies for dealing with novel situations. In the Cognitive Estimation Task (Shallice & Evans, 1978) patients are presented with questions whose answers are unlikely to be known. People with damage to the prefrontal cortex have major difficulties to produce estimates for questions like: “How many camels are in Holland?”.
In the FAS Test (Miller, 1984) subjects have to generate sequences of words (not proper names) beginning with a certain letter (“F” , “A” or “S”) in a one-minute period. This test involves developing new strategies, selecting between alternatives and avoiding repeating previous given answers. Patients with left lateral prefrontal lesions are often impaired (Stuss et al., 1998).
4. Technical difficulties or dangerous circumstances
One single mistake in a dangerous situation may easily lead to serious injuries while a mistake in a technical difficult situation (e.g. building a house of cards) would obviously lead to failure. Thus, in such situations, automatic activation of responses clearly would be insufficient and executive functions seem to be the only solution for such problems.
Wilkins, Shallice and McCarthy (1987) were able to prove a connection between dangerous or difficult situations and the prefrontal cortex, as patients with lesions to this area were impaired during experiments concerning dangerous or difficult situations. The ventromedial and orbitofrontal cortex may be particularly important for these aspects of executive functions.
5. Control of action or the overcoming of strong habitual responses
Deficits in initiation, cessation and control of action
We start by describing the effects of the loss of the ability to start something, to initiate an action. A person with executive dysfunction is likely to have trouble beginning to work on a task without strong help from the outside, while people with left frontal lobe damage often show impaired spontaneous speech and people with right frontal lobe damage rather show poor nonverbal fluency. Of course, one reason is the fact that this person will not have any intention, desire or concern on his or her own of solving the task since this is yet another characteristic of executive dysfunction. But it is also due to a psychological effect often connected with the loss of properly executive functioning: Psychological inertia. Like in physics, inertia in this case means that an action is very hard to initiate, but once started, it is again very hard to shift or stop. This phenomenon is characterized by engagement in repetitive behavior, is called perseveration (cp. WCST).
Another problem caused by executive dysfunction can be observed in patients suffering from the so called environmental dependency syndrome. Their actions are impelled or obligated by their physical or social environment. This manifests itself in many different ways and depends to a large extent on the individual’s personal history. Examples are patients who begin to type when they see a computer key board, who start washing the dishes upon seeing a dirty kitchen or who hang up pictures on the walls when finding hammer, nails and pictures on the floor. This makes these people appear as if they were acting impulsively or as if they have lost their ‘free will’. It shows a lack of control for their actions. This is due to the fact that an impairment in their executive functions causes a disconnection between thought and action. These patients know that their actions are inappropriate but like in the WCST, they cannot control what they are doing. Even if they are told by which attribute to sort the cards, they will still keep sorting them sticking to the old rule due to major difficulties in the translation of these directions into action.
What is needed to avoid problems like these are the abilities to start, stop or change an action but very likely also the ability to use information to direct behavior.
Deficits in cognitive estimation
Next to the difficulties to produce estimates to questions whose answers are unlikely known, patients with lesions to the frontal lobes have problems with cognitive estimation in general.
Cognitive estimation is the ability to use known information to make reasonable judgments or deductions about the world. Now the inability for cognitive estimation is the third type of deficits often observed in individuals with executive dysfunction. It is already known that people with executive dysfunction have a relatively unaffected knowledge base. This means they cannot retain knowledge about information or at least they are unable to make inferences based on it. There are various effects which are shown on such individuals. Now for example patients with frontal lobe damage have difficulty estimating the length of the spine of an average woman. Making such realistic estimations requires inferencing based on other knowledge which is in this case, knowing that the height of the average woman is about 5 ft 6 in (168 cm) and considering that the spine runs about one third to one half the length of the body and so on. Patients with such a dysfunction do not only have difficulties in their estimates of cognitive information but also in their estimates of their own capacities (such as their ability to direct activity in goal – oriented manner or in controlling their emotions). Prigatuno, Altman and O’Brien (1990) reported that when patients with anterior lesions associated with diffuse axonal injury to other brain areas are asked how capable they are of performing tasks such as scheduling their daily activities or preventing their emotions from affecting daily activities, they grossly overestimate their abilities. From several experiments Smith and Miler (1988) found out that individuals with frontal lobe damages have no difficulties in determining whether an item was in a specific inspection series they find it difficult to estimate how frequently an item did occur. This may not only reflect difficulties in cognitive estimation but also in memory task that place a premium on remembering temporal information. Thus both difficulties (in cognitive estimation and in temporal sequencing) may contribute to a reduced ability to estimate frequency of occurrence.
Despite these impairments in some domains the abilities of estimation are preserved in patients with frontal lobe damage. Such patients also do have problems in estimating how well they can prevent their emotions for affecting their daily activities. They are also as good at judging how many dues they will need to solve a puzzle as patients with temporal lobe damage or neurologically intact people.
Theories of frontal lobe function in executive control
In order to explain that patients with frontal lobe damage have difficulties in performing executive functions, four major approaches have developed. Each of them leads to an improved understanding of the role of frontal regions in executive functions, but none of these theories covers all the deficits occurred.
Role of working memory
The most anatomically specific approach assumes the dorsolateral prefrontal area of the frontal lobe to be critical for working memory. The working memory which has to be clearly distinguished from the long term memory keeps information on-line for use in performing a task. Not being generated for accounting for the broad array of dysfunctions it focuses on the three following deficits:
- Sequencing information and directing behavior toward a goal
- Understanding of temporal relations between items and events
- Some aspects of environmental dependency and perseveration
Research on monkeys has been helpful to develop this approach (the delayed-response paradigm, Goldman-Rakic, 1987, serves as a classical example).
Role of Controlled Versus Automatic Processes
There are two theories based on the underlying assumption that the frontal lobes are especially important for controlling behavior in non-experienced situations and for overriding stimulus-response associations, but contribute little to automatic and effortless behavior (Banich, 1997).
Stuss and Benson (1986) consider control over behavior to occur in a hierarchical manner. They distinguish between three different levels, of which each is associated with a particular brain region. In the first level sensory information is processed automatically by posterior regions, in the next level (associated with the executive functions of the frontal lobe) conscious control is needed to direct behavior toward a goal and at the highest level controlled self-reflection takes place in the prefrontal cortex.
This model is appropriate for explaining deficits in goal-oriented behavior, in dealing with novelty, the lack of cognitive flexibility and the environmental dependency syndrome. Furthermore it can explain the inability to control action consciously and to criticise oneself. The second model developed by Shalice (1982) proposes a system consisting of two parts that influence the choice of behavior. The first part, a cognitive system called contention scheduling, is in charge of more automatic processing. Various links and processing schemes cause a single stimulus to result in an automatic string of actions. Once an action is initiated, it remains active until inhibited. The second cognitive system is the supervisory attentional system which directs attention and guides action through decision processes and is only active “when no processing schemes are available, when the task is technically difficult, when problem solving is required and when certain response tendencies must be overcome” (Banich , 1997).
This theory supports the observations of few deficits in routine situations, but relevant problems in dealing with novel tasks (e.g. the Tower of London task, Shallice, 1982), since no schemes in contention scheduling exist for dealing with it. Impulsive action is another characteristic of patients with frontal lobe damages which can be explained by this theory. Even if asked not to do certain things, such patients stick to their routines and cannot control their automatic behavior.
Use of Scripts
The approach based on scripts, which are sets of events, actions and ideas that are linked to form a unit of knowledge was developed by Schank (1982) amongst others.
Containing information about the setting in which an event occurs, the set of events needed to achieve the goal and the end event terminating the action. Such managerial knowledge units (MKUs) are supposed to be stored in the prefrontal cortex. They are organized in a hierarchical manner being abstract at the top and getting more specific at the bottom.
Damage of the scripts leads to the inability to behave goal-directed, finding it easier to cope with usual situations (due to the difficulty of retrieving a MKU of a novel event) and deficits in the initiation and cessation of action (because of MKUs specifying the beginning and ending of an action.)
Role of a goal list
The perspective of artificial intelligence and machine learning introduced an approach which assumes that each person has a goal list, which contains the tasks requirements or goals. This list is fundamental to guiding behavior and since frontal lobe damages disrupt the ability to form a goal list, the theory helps to explain difficulties in abstract thinking, perceptual analysis, verbal output and staying on task. It can also account for the strong environmental influence on patients with frontal lobe damages, due to the lack of internal goals and the difficulty of organizing actions toward a goal.
| Brain Region | Possible Function (left hemisphere) | Possible Function (right hemisphere) | Brodman's Areas which are involved |
|---|---|---|---|
| ventrolateral prefrontal cortex (VLPFC) | Retrieval and maintenance of semantic and/or linguistic information | Retrieval and maintenance of visuospatial information | 44, 45, 47 (44 & 45 = Broca's Area) |
| dorsolateral prefrontal cortex )DLPRF) | Selecting a range of responses and suppressing inappropriate ones; manipulating the contents of working memory | Monitoring and checking of information held in mind, particularly in conditions of uncertainty; vigilance and sustained attention | 9, 46 |
| anterior prefrontal cortex; frontal pole; rostral prefrontal cortex | Multitasking; maintaining future intentions & goals while currently performing other tasks or subgoals | same | 10 |
| anterior cingulate cortex (dorsal) | Monitoring in situations of response conflict and error detection | same | 24 (dorsal) & 32 (dorsal) |