Discuss the importance of nutrition to early physical growth, including nutritional concerns for infants and toddlers such as marasmus and kwashiorkor
Good nutrition in a supportive environment is vital for an infant’s healthy growth and development. Remember, from birth to 1 year, infants triple their weight and increase their height by half, and this growth requires good nutrition. For the first 6 months, babies are fed breast milk or formula. Starting good nutrition practices early can help children develop healthy dietary patterns. Infants need to receive nutrients to fuel their rapid physical growth. Malnutrition during infancy can result in not only physical but also cognitive and social consequences. Without proper nutrition, infants cannot reach their physical potential.
Benefits of Breastfeeding
Figure 1. Breastmilk changes in composition with a newborn’s development and needs.
Breast milk is considered the ideal diet for newborns due to the nutritional makeup of colostrum and subsequent breastmilk production. Colostrum, the milk produced during pregnancy and just after birth, has been described as “liquid gold.” Colostrum is packed with nutrients and other important substances that help the infant build up his or her immune system. Most babies will get all the nutrition they need through colostrum during the first few days of life (CDC, 2018).[1] Breast milk changes by the third to fifth day after birth, becoming much thinner, but containing just the right amount of fat, sugar, water, and proteins to support overall physical and neurological development. It provides a source of iron more easily absorbed in the body than the iron found in dietary supplements, it provides resistance against many diseases, it is more easily digested by infants than formula, and it helps babies make a transition to solid foods more easily than if bottle-fed.
The reason infants need such a high fat content is the process of myelination which requires fat to insulate the neurons. There has been some research, including meta-analyses, to show that breastfeeding is connected to advantages with cognitive development (Anderson, Johnstone, & Remley, 1999)[2]. Low birth weight infants had the greatest benefits from breastfeeding than did normal-weight infants in a meta-analysis that of twenty controlled studies examining the overall impact of breastfeeding (Anderson et al., 1999). This meta-analysis showed that breastfeeding may provide nutrients required for rapid development of the immature brain and be connected to more rapid or better development of neurologic function. The studies also showed that a longer duration of breastfeeding was accompanied by greater differences in cognitive development between breastfed and formula-fed children. Whereas normal-weight infants showed a 2.66-point difference, low-birth-weight infants showed a 5.18-point difference in IQ compared with weight-matched, formula-fed infants (Anderson et al, 1999). These studies suggest that nutrients present in breast milk may have a significant effect on neurologic development in both premature and full-term infants.
Figure 2. Most children are introduced to solid foods around six months old, like this girl who is having her first taste of rice.
For most babies, breast milk is also easier to digest than formula. Formula-fed infants experience more diarrhea and upset stomachs. The absence of antibodies in formula often results in a higher rate of ear infections and respiratory infections. Children who are breastfed have lower rates of childhood leukemia, asthma, obesity, type 1 and 2 diabetes, and a lower risk of SIDS. For all of these reasons, it is recommended that mothers breastfeed their infants until at least 6 months of age and that breast milk be used in the diet throughout the first year (U.S. Department of Health and Human Services, 2004a in Berk, 2007).
Several recent studies have reported that it is not just babies that benefit from breastfeeding. Breastfeeding stimulates contractions in the uterus to help it regain its normal size, and women who breastfeed are more likely to space their pregnancies farther apart. Mothers who breastfeed are at lower risk of developing breast cancer, especially among higher-risk racial and ethnic groups (Islami et al., 2015).[3] Other studies suggest that women who breastfeed have lower rates of ovarian cancer (Titus-Ernstoff, Rees, Terry, & Cramer, 2010)[4], and reduced risk for developing Type 2 diabetes (Gunderson, et al., 2015)[5], and rheumatoid arthritis (Karlson, Mandl, Hankinson, & Grodstein, 2004).[6]
A historic look at breastfeeding
The use of wet nurses, or lactating women, hired to nurse others’ infants, during the middle ages eventually declined, and mothers increasingly breastfed their own infants in the late 1800s. In the early part of the 20th century, breastfeeding began to go through another decline, and by the 1950s it was practiced less frequently by middle class, more affluent mothers as formula began to be viewed as superior to breast milk. In the late 1960s and 1970s, there was again a greater emphasis placed on natural childbirth and breastfeeding and the benefits of breastfeeding were more widely publicized. Gradually, rates of breastfeeding began to climb, particularly among middle-class educated mothers who received the strongest messages to breastfeed.
Today, new mothers receive consultation from lactation specialists before being discharged from the hospital to ensure that they are informed of the benefits of breastfeeding and given support and encouragement to get their infants accustomed to taking the breast. This does not always happen immediately, and first-time mothers, especially, can become upset or discouraged. In this case, lactation specialists and nursing staff can encourage the mother to keep trying until the baby and mother are comfortable with the feeding.
Most mothers who breastfeed in the United States stop breastfeeding at about 6-8 weeks, often in order to return to work outside the home (United States Department of Health and Human Services (USDHHS), 2011[7]). Mothers can certainly continue to provide breast milk to their babies by expressing and freezing the milk to be bottle fed at a later time or by being available to their infants at feeding time, but some mothers find that after the initial encouragement they receive in the hospital to breastfeed, the outside world is less supportive of such efforts. Some workplaces support breastfeeding mothers by providing flexible schedules and welcoming infants, but many do not. And the public support of breastfeeding is sometimes lacking. Women in Canada are more likely to breastfeed than are those in the United States, and the Canadian health recommendation is for breastfeeding to continue until 2 years of age. Facilities in public places in Canada such as malls, ferries, and workplaces provide more support and comfort for the breastfeeding mother and child than found in the United States.
In addition to the nutritional and health benefits of breastfeeding, breast milk is free! Anyone who has priced formula recently can appreciate this added incentive to breastfeeding. Prices for a month’s worth of formula can easily range from $130-$200. Prices for a year’s worth of formula and feeding supplies can cost well over $1,500 (USDHHS, 2011).
Links to Learning
Watch this video from the Psych SciShow “Bad Science: Breastmilk and Formula” to learn about research related to both breastfeeding and formula-feeding.
To learn more about breastfeeding, visit this resource from the U.S. Department of Health and Human Resources: Your Guide to Breastfeeding.
Visit Kids Health on Breastfeeding vs. Formula Feeding to learn more about the benefits and challenges of each. Click on the speaker icon to listen to the narration of the article if you would like.
When Breastfeeding Doesn’t Work
There are occasions where mothers may be unable to breastfeed babies, often for a variety of health, social, and emotional reasons. For example, breastfeeding generally does not work:
when the baby is adopted
when the biological mother has a transmissible disease such as tuberculosis or HIV
when the mother is addicted to drugs or taking any medication that may be harmful to the baby (including some types of birth control)
when the infant was born to (or adopted by) a family with two fathers and the surrogate mother is not available to breastfeed
when there are attachment issues between mother and baby
when the mother or the baby is in the Intensive Care Unit (ICU) after the delivery process
when the baby and mother are attached but the mother does not produce enough breast-milk
One early argument given to promote the practice of breastfeeding (when health issues are not the case) is that it promotes bonding and healthy emotional development for infants. However, this does not seem to be a unique case. Breastfed and bottle-fed infants adjust equally well emotionally (Ferguson & Woodward, 1999). This is good news for mothers who may be unable to breastfeed for a variety of reasons and for fathers who might feel left out as a result.
Breast milk or formula is the only food a newborn needs, and the American Academy of Pediatrics recommends exclusive breastfeeding for the first six months after birth. Solid foods can be introduced from around six months onward when babies develop stable sitting and oral feeding skills but should be used only as a supplement to breast milk or formula. By six months, the gastrointestinal tract has matured, solids can be digested more easily, and allergic responses are less likely. The infant is also likely to develop teeth around this time, which aids in chewing solid food. Iron-fortified infant cereal, made of rice, barley, or oatmeal, is typically the first solid introduced due to its high iron content. Cereals can be made of rice, barley, or oatmeal. Generally, salt, sugar, processed meat, juices, and canned foods should be avoided.
Though infants usually start eating solid foods between 4 and 6 months of age, more and more solid foods are consumed by a growing toddler. Pediatricians recommended introducing foods one at a time, and for a few days, in order to identify any potential food allergies. Toddlers may be picky at times, but it remains important to introduce a variety of foods and offer food with essential vitamins and nutrients, including iron, calcium, and vitamin D.
Milk Anemia in the United States
About 9 million children in the United States are malnourished (Children’s Welfare, 1998). More still suffer from milk anemia, a condition in which milk consumption leads to a lack of iron in the diet. The prevalence of iron deficiency anemia in 1- to 3-year-old children seems to be increasing (Kazal, 2002)[8]. The body gets iron through certain foods. Toddlers who drink too much cow’s milk may also become anemic if they are not eating other healthy foods that have iron. This can be due to the practice of giving toddlers milk as a pacifier when resting, riding, walking, and so on. Appetite declines somewhat during toddlerhood and a small amount of milk (especially with added chocolate syrup) can easily satisfy a child’s appetite for many hours. The calcium in milk interferes with the absorption of iron in the diet as well. There is also a link between iron deficiency anemia and diminished mental, motor, and behavioral development. In the second year of life, iron deficiency can be prevented by the use of a diversified diet that is rich in sources of iron and vitamin C, limiting cow’s milk consumption to less than 24 ounces per day, and providing a daily iron-fortified vitamin.
Global Considerations and Malnutrition
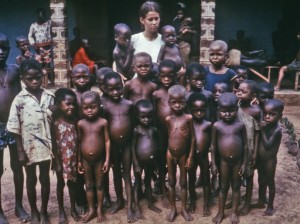
Figure 3. These children are showing the extended abdomen characteristic of kwashiorkor (Photo Courtesy Centers for Disease Control and Prevention).
In the 1960s, formula companies led campaigns in developing countries to encourage mothers to feed their babies on infant formula. Many mothers felt that formula would be superior to breast milk and began using formula. The use of formula can certainly be healthy under conditions in which there is adequate, clean water with which to mix the formula and adequate means to sanitize bottles and nipples. However, in many of these countries, such conditions were not available and babies often were given diluted, contaminated formula which made them become sick with diarrhea and become dehydrated. These conditions continue today and now many hospitals prohibit the distribution of formula samples to new mothers in efforts to get them to rely on breastfeeding. Many of these mothers do not understand the benefits of breastfeeding and have to be encouraged and supported in order to promote this practice.
The World Health Organization (2018) recommends:
initiation of breastfeeding within one hour of birth
exclusive breastfeeding for the first six months of life
introduction of solid foods at six months together with continued breastfeeding up to two years of age or beyond
Link to Learning
Breastfeeding could save the lives of millions of infants each year, according to the World Health Organization (WHO), yet fewer than 40 percent of infants are breastfed exclusively for the first 6 months of life. Most women can breastfeed unless they are receiving chemotherapy or radiation therapy, have HIV, are dependent on illicit drugs, or have active untreated tuberculosis. Because of the great benefits of breastfeeding, WHO, UNICEF and other national organizations are working together with the government to step up support for breastfeeding globally.
Children in developing countries and countries experiencing the harsh conditions of war are at risk for two major types of malnutrition. Infantile marasmus refers to starvation due to a lack of calories and protein. Children who do not receive adequate nutrition lose fat and muscle until their bodies can no longer function. Babies who are breastfed are much less at risk of malnutrition than those who are bottle-fed. After weaning, children who have diets deficient in protein may experience kwashiorkor, or the “disease of the displaced child,” often occurring after another child has been born and taken over breastfeeding. This results in a loss of appetite and swelling of the abdomen as the body begins to break down the vital organs as a source of protein.
Watch It
Watch this video to learn more about the signs and symptoms of kwashiorkor and marasmus.
A link to an interactive elements can be found at the bottom of this page.
the first secretion from the mammary glands after giving birth, rich in antibodies
infantile marasmus
starvation due to a lack of calories and protein
kwashiorkor
also known as the “disease of the displaced child,” results in a loss of appetite and swelling of the abdomen as the body begins to break down the vital organs as a source of protein
malnutrition
a condition that results from eating a diet in which one or more nutrients are deficient
milk anemia
an iron deficiency in infants who have been maintained on a milk diet for too long
Islami, F., Liu, Y., Jemal, A., Zhou, J., Weiderpass, E., Colditz, G., Boffetta, P., & Weiss, M. (2015). Breastfeeding and breast cancer risks by receptor status- a systematic review and meta-analysis. Annals of Oncology, 26,12. 2398–2407. mailto:/Sandboxes/lhrli@ucdavis.edu
Titus-Ernstoff, Rees, L. Terry, R.R., & Cramer, D. W. (2010). Breast-feeding the last born child and risk of ovarian cancer. Cancer Causes Control. 21(2), 201–207. mailto:/Sandboxes/lhrli@ucdavis.edu
Gunderson, E.P., Hurston, S.R., Dewey, K.G., Faith, M.S., Charvat-Aguilar, N., Khoury, V. C., Nguyen, V.T., & Quesenberry, C.P. (2015). The study of women, infant feeding and type 2 diabetes after GDM pregnancy and growth of their offspring (SWIFT Offspring study): prospective design, methodology and baseline characteristics. BMC Pregnancy and Childbirth, 15,150 https://doi.org/10.1186/s12884-015-0587-zmailto:/Sandboxes/lhrli@ucdavis.edu
Karlson, E.W., Mandl, L.A., Hankinson, S. E., & Grodstein, F. (2004). Do breast-feeding and other reproductive factors influence future risk of rheumatoid arthritis? Results from the Nurses' Health Study. Arthritis Rheum. 50,11, 3458-67. mailto:/Sandboxes/lhrli@ucdavis.edu
United States Department of Health and Human Services, Office of Women’s Health (2011). Your guide to breast feeding. Washington D.C. mailto:/Sandboxes/lhrli@ucdavis.edu
KAZAL, L.A. (2002). Navajo Health Foundation/Sage Memorial Hospital, Ganado, Arizona Am Fam Physician. 66(7): 1217-1225. mailto:/Sandboxes/lhrli@ucdavis.edu
Contributors and Attributions
CC licensed content, Original
Modification, adaptation, and original content. Authored by: Tera Jones for Lumen Learning. Provided by: Lumen Learning. License: CC BY: Attribution
Child Malnutrition - What? How? And when to Refer. Provided by: iheed. Located at: https://www.youtube.com/watch?v=bqEIcMMmj5M. License: Other. License Terms: Standard YouTube License