The purpose of this module is to define what is meant by a personality disorder, identify the five domains of general personality (i.e., neuroticism, extraversion, openness, agreeableness, and conscientiousness), identify the six personality disorders proposed for retention in the 5th edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) (i.e., borderline, antisocial, schizotypal, avoidant, obsessive-compulsive, and narcissistic), summarize the etiology for antisocial and borderline personality disorder, and identify the treatment for borderline personality disorder (i.e., dialectical behavior therapy and mentalization therapy).
learning objectives
Define what is meant by a personality disorder.
Identify the five domains of general personality.
Identify the six personality disorders proposed for retention in DSM-5.
Summarize the etiology for antisocial and borderline personality disorder.
Identify the treatment for borderline personality disorder.
Introduction
Everybody has their own unique personality; that is, their characteristic manner of thinking, feeling, behaving, and relating to others (John, Robins, & Pervin, 2008). Some people are typically introverted, quiet, and withdrawn; whereas others are more extraverted, active, and outgoing. Some individuals are invariably conscientiousness, dutiful, and efficient; whereas others might be characteristically undependable and negligent. Some individuals are consistently anxious, self-conscious, and apprehensive; whereas others are routinely relaxed, self-assured, and unconcerned. Personality traits refer to these characteristic, routine ways of thinking, feeling, and relating to others. There are signs or indicators of these traits in childhood, but they become particularly evident when the person is an adult. Personality traits are integral to each person’s sense of self, as they involve what people value, how they think and feel about things, what they like to do, and, basically, what they are like most every day throughout much of their lives.
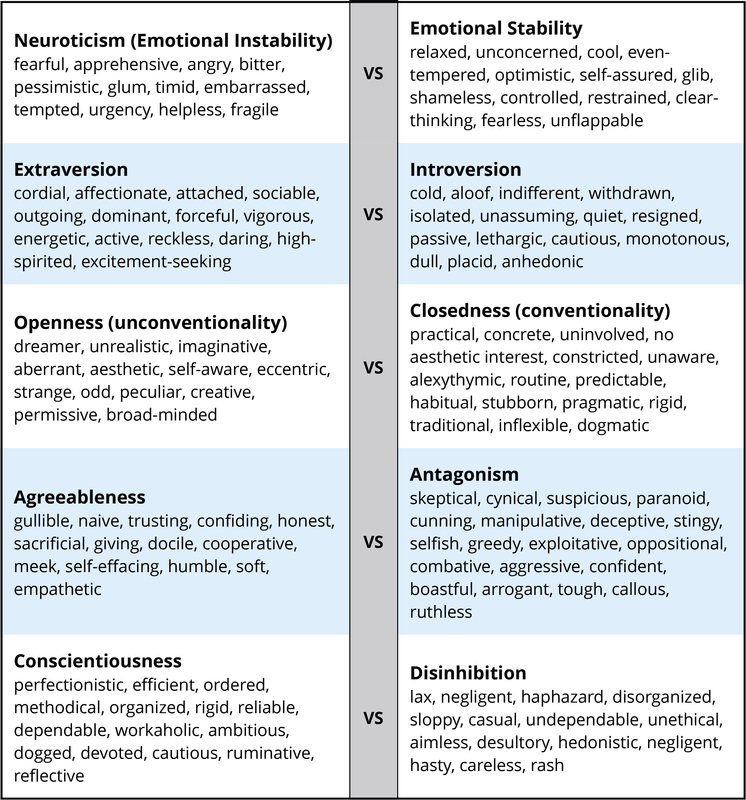
There are literally hundreds of different personality traits. All of these traits can be organized into the broad dimensions referred to as the Five-Factor Model (John, Naumann, & Soto, 2008). These five broad domains are inclusive; there does not appear to be any traits of personality that lie outside of the Five-Factor Model. This even applies to traits that you may use to describe yourself. Table I provides illustrative traits for both poles of the five domains of this model of personality. A number of the traits that you see in this table may describe you. If you can think of some other traits that describe yourself, you should be able to place them somewhere in this table.
Table I: Illustrative traits for both poles across Five-Factor Model personality dimensions.
DSM-5 Personality Disorders
When personality traits result in significant distress, social impairment, and/or occupational impairment, they are considered to be a personality disorder (American Psychiatric Association, 2013). The authoritative manual for what constitutes a personality disorder is provided by the American Psychiatric Association’s (APA) Diagnostic and Statistical Manual of Mental Disorders (DSM), the current version of which is DSM-5 (APA, 2013). The DSM provides a common language and standard criteria for the classification and diagnosis of mental disorders. This manual is used by clinicians, researchers, health insurance companies, and policymakers. DSM-5 includes 10 personality disorders: antisocial, avoidant, borderline, dependent, histrionic, narcissistic, obsessive-compulsive, paranoid, schizoid, and schizotypal. All 10 of these personality disorders will be included in the next edition of the diagnostic manual, DSM-5.
This list of 10 though does not fully cover all of the different ways in which a personality can be maladaptive. DSM-5 also includes a “wastebasket” diagnosis of other specified personality disorder (OSPD) and unspecified personality disorder (UPD). This diagnosis is used when a clinician believes that a patient has a personality disorder but the traits that constitute this disorder are not well covered by one of the 10 existing diagnoses. OSPD and UPD or as they used to be referred to in previous editions - PDNOS (personality disorder not otherwise specified) are often one of the most frequently used diagnoses in clinical practice, suggesting that the current list of 10 is not adequately comprehensive (Widiger & Trull, 2007).
Description
Each of the 10 DSM-5 (and DSM-IV-TR) personality disorders is a constellation of maladaptive personality traits, rather than just one particular personality trait (Lynam & Widiger, 2001). In this regard, personality disorders are “syndromes.” For example, avoidant personality disorder is a pervasive pattern of social inhibition, feelings of inadequacy, and hypersensitivity to negative evaluation (APA, 2013), which is a combination of traits from introversion (e.g., socially withdrawn, passive, and cautious) and neuroticism (e.g., self-consciousness, apprehensiveness, anxiousness, and worrisome). Dependent personality disorder includes submissiveness, clinging behavior, and fears of separation (APA, 2013), for the most part a combination of traits of neuroticism (anxious, uncertain, pessimistic, and helpless) and maladaptive agreeableness (e.g., gullible, guileless, meek, subservient, and self-effacing). Antisocial personality disorder is, for the most part, a combination of traits from antagonism (e.g., dishonest, manipulative, exploitative, callous, and merciless) and low conscientiousness (e.g., irresponsible, immoral, lax, hedonistic, and rash). See the 1967 movie, Bonnie and Clyde, starring Warren Beatty, for a nice portrayal of someone with antisocial personality disorder.
A person with an obsessive compulsive personality disorder may have a hard time relaxing, always feel under pressure, and believe that there isn't enough time to accomplish important tasks. [Image: CC0 Public Domain, goo.gl/m25gce]
Some of the DSM-5 personality disorders are confined largely to traits within one of the basic domains of personality. For example, obsessive-compulsive personality disorder is largely a disorder of maladaptive conscientiousness, including such traits as workaholism, perfectionism, punctilious, ruminative, and dogged; schizoid is confined largely to traits of introversion (e.g., withdrawn, cold, isolated, placid, and anhedonic); borderlinepersonality disorder is largely a disorder of neuroticism, including such traits as emotionally unstable, vulnerable, overwhelmed, rageful, depressive, and self-destructive (watch the 1987 movie, Fatal Attraction, starring Glenn Close, for a nice portrayal of this personality disorder); and histrionic personality disorder is largely a disorder of maladaptive extraversion, including such traits as attention-seeking, seductiveness, melodramatic emotionality, and strong attachment needs (see the 1951 film adaptation of Tennessee William’s play, Streetcar Named Desire, starring Vivian Leigh, for a nice portrayal of this personality disorder).
It should be noted though that a complete description of each DSM-5 personality disorder would typically include at least some traits from other domains. For example, antisocial personality disorder (or psychopathy) also includes some traits from low neuroticism (e.g., fearlessness and glib charm) and extraversion (e.g., excitement-seeking and assertiveness); borderline includes some traits from antagonism (e.g., manipulative and oppositional) and low conscientiousness (e.g., rash); and histrionic includes some traits from antagonism (e.g., vanity) and low conscientiousness (e.g., impressionistic). Narcissistic personality disorder includes traits from neuroticism (e.g., reactive anger, reactive shame, and need for admiration), extraversion (e.g., exhibitionism and authoritativeness), antagonism (e.g., arrogance, entitlement, and lack of empathy), and conscientiousness (e.g., acclaim-seeking). Schizotypal personality disorder includes traits from neuroticism (e.g., social anxiousness and social discomfort), introversion (e.g., social withdrawal), unconventionality (e.g., odd, eccentric, peculiar, and aberrant ideas), and antagonism (e.g., suspiciousness).
The APA currently conceptualizes personality disorders as qualitatively distinct conditions; distinct from each other and from normal personality functioning. However, included within an appendix to DSM-5 is an alternative view that personality disorders are simply extreme and/or maladaptive variants of normal personality traits, as suggested herein. Nevertheless, many leading personality disorder researchers do not hold this view (e.g., Gunderson, 2010; Hopwood, 2011; Shedler et al., 2010). They suggest that there is something qualitatively unique about persons suffering from a personality disorder, usually understood as a form of pathology in sense of self and interpersonal relatedness that is considered to be distinct from personality traits (APA, 2012; Skodol, 2012). For example, it has been suggested that antisocial personality disorder includes impairments in identity (e.g., egocentrism), self-direction, empathy, and capacity for intimacy, which are said to be different from such traits as arrogance, impulsivity, and callousness (APA, 2012).
Validity
It is quite possible that in future revisions of the DSM some of the personality disorders included in DSM-5 and DSM-IV-TR will no longer be included. In fact, for DSM-5 it was originally proposed that four be deleted. The personality disorders that were slated for deletion were histrionic, schizoid, paranoid, and dependent (APA, 2012). The rationale for the proposed deletions was in large part because they are said to have less empirical support than the diagnoses that were at the time being retained (Skodol, 2012). There is agreement within the field with regard to the empirical support for the borderline, antisocial, and schizotypal personality disorders (Mullins-Sweat, Bernstein, & Widiger, 2012; Skodol, 2012). However, there is a difference of opinion with respect to the empirical support for the dependent personality disorder (Bornstein, 2012; Livesley, 2011; Miller, Widiger, & Campbell, 2010; Mullins-Sweat et al., 2012).
Little is known about the specific etiology for most of the DSM-5 personality disorders. Because each personality disorder represents a constellation of personality traits, the etiology for the syndrome will involve a complex interaction of an array of different neurobiological vulnerabilities and dispositions with a variety of environmental, psychosocial events. Antisocial personality disorder, for instance, is generally considered to be the result of an interaction of genetic dispositions for low anxiousness, aggressiveness, impulsivity, and/or callousness, with a tough, urban environment, inconsistent parenting, poor parental role modeling, and/or peer support (Hare, Neumann, & Widiger, 2012). Borderline personality disorder is generally considered to be the result of an interaction of a genetic disposition to negative affectivity interacting with a malevolent, abusive, and/or invalidating family environment (Hooley, Cole, & Gironde, 2012).
To the extent that one considers the DSM-5 personality disorders to be maladaptive variants of general personality structure, as described, for instance, within the Five-Factor Model, there would be a considerable body of research to support the validity for all of the personality disorders, including even the histrionic, schizoid, and paranoid. There is compelling multivariate behavior genetic support with respect to the precise structure of the Five-Factor Model (e.g., Yamagata et al., 2006), childhood antecedents (Caspi, Roberts, & Shiner, 2005), universality (Allik, 2005), temporal stability across the lifespan (Roberts & DelVecchio, 2000), ties with brain structure (DeYoung, Hirsh, Shane, Papademetris, Rajeevan, & Gray, 2010), and even molecular genetic support for neuroticism (Widiger, 2009).
Treatment
Personality disorders are relatively unique because they are often “ego-syntonic;” that is, most people are largely comfortable with their selves, with their characteristic manner of behaving, feeling, and relating to others. As a result, people rarely seek treatment for their antisocial, narcissistic, histrionic, paranoid, and/or schizoid personality disorder. People typically lack insight into the maladaptivity of their personality.
Many people with personality disorders do not seek treatment. Those with borderline personality disorder and avoidant personality disorder are exceptions. High levels of neuroticism and emotional pain may motivate them to seek help. [Image: CC0 Public Domain, goo.gl/m25gce]
One clear exception though is borderline personality disorder (and perhaps as well avoidant personality disorder). Neuroticism is the domain of general personality structure that concerns inherent feelings of emotional pain and suffering, including feelings of distress, anxiety, depression, self-consciousness, helplessness, and vulnerability. Persons who have very high elevations on neuroticism (i.e., persons with borderline personality disorder) experience life as one of pain and suffering, and they will seek treatment to alleviate this severe emotional distress. People with avoidant personality may also seek treatment for their high levels of neuroticism (anxiousness and self-consciousness) and introversion (social isolation). In contrast, narcissistic individuals will rarely seek treatment to reduce their arrogance; paranoid persons rarely seek treatment to reduce their feelings of suspiciousness; and antisocial people rarely (or at least willfully) seek treatment to reduce their disposition for criminality, aggression, and irresponsibility.
Nevertheless, maladaptive personality traits will be evident in many individuals seeking treatment for other mental disorders, such as anxiety, mood, or substance use. Many of the people with a substance use disorder will have antisocial personality traits; many of the people with mood disorder will have borderline personality traits. The prevalence of personality disorders within clinical settings is estimated to be well above 50% (Torgersen, 2012). As many as 60% of inpatients within some clinical settings are diagnosed with borderline personality disorder (APA, 2000). Antisocial personality disorder may be diagnosed in as many as 50% of inmates within a correctional setting (Hare et al., 2012). It is estimated that 10% to 15% of the general population meets criteria for at least one of the 10 DSM-IV-TR personality disorders (Torgersen, 2012), and quite a few more individuals are likely to have maladaptive personality traits not covered by one of the 10 DSM-5 diagnoses.
The presence of a personality disorder will often have an impact on the treatment of other mental disorders, typically inhibiting or impairing responsivity. Antisocial persons will tend to be irresponsible and negligent; borderline persons can form intensely manipulative attachments to their therapists; paranoid patients will be unduly suspicious and accusatory; narcissistic patients can be dismissive and denigrating; and dependent patients can become overly attached to and feel helpless without their therapists.
It is a misnomer, though, to suggest that personality disorders cannot themselves be treated. Personality disorders are among the most difficult of disorders to treat because they involve well-established behaviors that can be integral to a client’s self-image (Millon, 2011). Nevertheless, much has been written on the treatment of personality disorder (e.g., Beck, Freeman, Davis, & Associates, 1990; Gunderson & Gabbard, 2000), and there is empirical support for clinically and socially meaningful changes in response to psychosocial and pharmacologic treatments (Perry & Bond, 2000). The development of an ideal or fully healthy personality structure is unlikely to occur through the course of treatment, but given the considerable social, public health, and personal costs associated with some of the personality disorders, such as the antisocial and borderline, even just moderate adjustments in personality functioning can represent quite significant and meaningful change.
Nevertheless, manualized and/or empirically validated treatment protocols have been developed for only one personality disorder, borderline (APA, 2001).
Focus Topic: Treatment of Borderline Personality Disorder
Dialectical behavior therapy (Lynch & Cuyper, 2012) and mentalization therapy (Bateman & Fonagy, 2012): Dialectical behavior therapy is a form of cognitive-behavior therapy that draws on principles from Zen Buddhism, dialectical philosophy, and behavioral science. The treatment has four components: individual therapy, group skills training, telephone coaching, and a therapist consultation team, and will typically last a full year. As such, it is a relatively expensive form of treatment, but research has indicated that its benefits far outweighs its costs, both financially and socially.
It is unclear why specific and explicit treatment manuals have not been developed for the other personality disorders. This may reflect a regrettable assumption that personality disorders are unresponsive to treatment. It may also reflect the complexity of their treatment. As noted earlier, each DSM-5 disorder is a heterogeneous constellation of maladaptive personality traits. In fact, a person can meet diagnostic criteria for the antisocial, borderline, schizoid, schizotypal, narcissistic, and avoidant personality disorders and yet have only one diagnostic criterion in common. For example, only five of nine features are necessary for the diagnosis of borderline personality disorder; therefore, two persons can meet criteria for this disorder and yet have only one feature in common. In addition, patients meeting diagnostic criteria for one personality disorder will often meet diagnostic criteria for another. This degree of diagnostic overlap and heterogeneity of membership hinders tremendously any effort to identify a specific etiology, pathology, or treatment for a respective personality disorder as there is so much variation within any particular group of patients sharing the same diagnosis (Smith & Zapolski, 2009).
Of course, this diagnostic overlap and complexity did not prevent researchers and clinicians from developing dialectical behavior therapy and mentalization therapy. A further reason for the weak progress in treatment development is that, as noted earlier, persons rarely seek treatment for their personality disorder. It would be difficult to obtain a sufficiently large group of people with, for instance, narcissistic or obsessive–compulsive disorder to participate in a treatment outcome study, one receiving the manualized treatment protocol, the other receiving treatment as usual.
Conclusions
It is evident that all individuals have a personality, as indicated by their characteristic way of thinking, feeling, behaving, and relating to others. For some people, these traits result in a considerable degree of distress and/or impairment, constituting a personality disorder. A considerable body of research has accumulated to help understand the etiology, pathology, and/or treatment for some personality disorders (i.e., antisocial, schizotypal, borderline, dependent, and narcissistic), but not so much for others (e.g., histrionic, schizoid, and paranoid). However, researchers and clinicians are now shifting toward a more dimensional understanding of personality disorders, wherein each is understood as a maladaptive variant of general personality structure, thereby bringing to bear all that is known about general personality functioning to an understanding of these maladaptive variants.
Do you think that any of the personality disorders, or some of their specific traits, are ever good or useful to have?
If someone with a personality disorder commits a crime, what is the right way for society to respond? For example, does or should meeting diagnostic criteria for antisocial personality disorder mitigate (lower) a person’s responsibility for committing a crime?
Given what you know about personality disorders and the traits that comprise each one, would you say there is any personality disorder that is likely to be diagnosed in one gender more than the other? Why or why not?
Do you believe that personality disorders can be best understood as a constellation of maladaptive personality traits, or do you think that there is something more involved for individuals suffering from a personality disorder?
The authors suggested Clyde Barrow as an example of antisocial personality disorder and Blanche Dubois for histrionic personality disorder. Can you think of a person from the media or literature who would have at least some of the traits of narcissistic personality disorder?
Vocabulary
Antisocial
A pervasive pattern of disregard and violation of the rights of others. These behaviors may be aggressive or destructive and may involve breaking laws or rules, deceit or theft.
Avoidant
A pervasive pattern of social inhibition, feelings of inadequacy, and hypersensitivity to negative evaluation.
Borderline
A pervasive pattern of instability of interpersonal relationships, self-image, and affects, and marked impulsivity.
Dependent
A pervasive and excessive need to be taken care of that leads to submissive and clinging behavior and fears of separation.
Five-Factor Model
Five broad domains or dimensions that are used to describe human personality.
Histrionic
A pervasive pattern of excessive emotionality and attention seeking.
Narcissistic
A pervasive pattern of grandiosity (in fantasy or behavior), need for admiration, and lack of empathy.
Obsessive-compulsive
A pervasive pattern of preoccupation with orderliness, perfectionism, and mental and interpersonal control, at the expense of flexibility, openness, and efficiency.
Paranoid
A pervasive distrust and suspiciousness of others such that their motives are interpreted as malevolent.
Personality
Characteristic, routine ways of thinking, feeling, and relating to others.
Personality disorders
When personality traits result in significant distress, social impairment, and/or occupational impairment.
Schizoid
A pervasive pattern of detachment from social relationships and a restricted range of expression of emotions in interpersonal settings.
Schizotypal
A pervasive pattern of social and interpersonal deficits marked by acute discomfort with, and reduced capacity for, close relationships as well as perceptual distortions and eccentricities of behavior.
References
Allik, J. (2005). Personality dimensions across cultures. Journal of Personality Disorders, 19, 212–232.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders: DSM-5.Washington, D.C: American Psychiatric Association.
American Psychiatric Association. (2001). Practice guidelines for the treatment of patients with borderline personality disorder. Washington, DC: Author.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed., text rev.) Washington, D.C: American Psychiatric Association.
Bateman, A. W., & Fonagy, P. (2012). Mentalization-based treatment of borderline personality disorder. In T. A. Widiger (Ed.), The Oxford handbook of personality disorders (pp. 767–784). New York, NY: Oxford University Press.
Beck, A. T., Freeman, A., Davis, D., and Associates (1990). Cognitive therapy of personality disorders, (2nd ed.). New York, NY: Guilford Press.
Bornstein, R. F. (2012). Illuminating a neglected clinical issue: Societal costs of interpersonal dependency and dependent personality disorder. Journal of Clinical Psychology, 68, 766–781.
Caspi, A., Roberts, B. W., & Shiner, R. L. (2005). Personality development: Stability and change. Annual Review of Psychology, 56, 453–484.
DeYoung, C. G., Hirsh, J. B., Shane, M. S., Papademetris, X., Rajeevan, N., & Gray, J. (2010). Testing predictions from personality neuroscience: Brain structure and the Big Five. Psychological Science, 21, 820–828.
Gunderson, J. G. (2010). Commentary on “Personality traits and the classification of mental disorders: Toward a more complete integration in DSM-5 and an empirical model of psychopathology.” Personality Disorders: Theory, Research, and Treatment, 1, 119–122.
Gunderson, J. G., & Gabbard, G. O. (Eds.), (2000). Psychotherapy for personality disorders. Washington, DC: American Psychiatric Press.
Hare, R. D., Neumann, C. S., & Widiger, T. A. (2012). Psychopathy. In T. A. Widiger (Ed.), The Oxford handbook of personality disorders (pp. 478–504). New York, NY: Oxford University Press.
Hooley, J. M., Cole, S. H., & Gironde, S. (2012). Borderline personality disorder. In T. A. Widiger (Ed.), The Oxford handbook of personality disorders (pp. 409–436). New York, NY: Oxford University Press.
Hopwood, C. J. (2011). Personality traits in the DSM-5. Journal of Personality Assessment, 93, 398–405.
John, O. P., Naumann, L. P., & Soto, C. J. (2008). Paradigm shift to the integrative Big Five trait taxonomy: History, measurement, and conceptual issues. In O. P. John, R. R. Robins, & L. A. Pervin (Eds.), Handbook of personality. Theory and research (3rd ed., pp. 114–158). New York, NY: Guilford Press.
John, O. P., Robins, R. W., & Pervin, L. A. (Eds.), (2008). Handbook of personality. Theory and Research (3rd ed.). New York, NY: Guilford Press.
Livesley, W. J. (2011). Confusion and incoherence in the classification of personality disorder: Commentary on the preliminary proposals for DSM-5. Psychological Injury and Law, 3, 304–313.
Lynam, D. R., & Widiger, T. A. (2001). Using the five factor model to represent the DSM-IV personality disorders: An expert consensus approach. Journal of Abnormal Psychology, 110, 401–412.
Lynch, T. R., & Cuper, P. F. (2012). Dialectical behavior therapy of borderline and other personality disorders. In T. A. Widiger (Ed.), The Oxford handbook of personality disorders (pp. 785–793). New York, NY: Oxford University Press.
Miller, J. D., Widiger, T. A., & Campbell, W. K. (2010). Narcissistic personality disorder and the DSM-V. Journal of Abnormal Psychology, 119, 640–649.
Millon, T. (2011). Disorders of personality. Introducing a DSM/ICD spectrum from normal to abnormal (3rd ed.). New York, NY: John Wiley & Sons.
Mullins-Sweatt; Bernstein; Widiger. Retention or deletion of personality disorder diagnoses for DSM-5: an expert consensus approach. Journal of personality disorders 2012;26(5):689-703.
Perry, J. C., & Bond, M. (2000). Empirical studies of psychotherapy for personality disorders. In J. Gunderson and G. Gabbard (Eds.), Psychotherapy for personality disorders (pp. 1–31). Washington DC: American Psychiatric Press.
Roberts, B. W., & DelVecchio, W. F. (2000). The rank-order consistency of personality traits from childhood to old age: A quantitative review of longitudinal studies. Psychological Bulletin, 126, 3–25.
Shedler, J., Beck, A., Fonagy, P., Gabbard, G. O., Gunderson, J. G., Kernberg, O., ... Westen, D. (2010). Personality disorders in DSM-5. American Journal of Psychiatry, 167, 1027–1028.
Skodol, A. (2012). Personality disorders in DSM-5. Annual Review of Clinical Psychology, 8, 317–344.
Smith, G. G., & Zapolski, T. C. B. (2009). Construct validation of personality measures. In J. N. Butcher (Ed.), The Oxford Handbook of Personality Assessment (pp. 81–98). New York, NY: Oxford University Press.
Torgerson, S. (2012). Epidemiology. In T. A. Widiger (Ed.), The Oxford handbook of personality disorders (pp. 186–205). New York, NY: Oxford University Press.
Widiger, T. A. (2009). Neuroticism. In M. R. Leary and R.H. Hoyle (Eds.), Handbook of individual differences in social behavior (pp. 129–146). New York, NY: Guilford Press.
Widiger, T. A., & Trull, T. J. (2007). Plate tectonics in the classification of personality disorder: Shifting to a dimensional model. American Psychologist, 62, 71–83.
Yamagata, S., Suzuki, A., Ando, J., One, Y., Kijima, N., Yoshimura, K., … Jang, K. L. (2006). Is the genetic structure of human personality universal? A cross-cultural twin study from North America, Europe, and Asia. Journal of Personality and Social Psychology, 90, 987–998.