Explain what determines the chromosomal sex of the child.
Question the assertion that human traits are genetic.
Compare monozygotic and dizygotic twins.
Differentiate between genetic disorders and chromosomal abnormalities.
Describe Trisomy 21.
Differentiate between the germinal, embryonic, and fetal periods of development.
Describe human development during the germinal, embryonic, and fetal periods.
Describe a normal delivery and complications of pregnancy and delivery.
Predict the risks to prenatal development posed by exposure to teratogens.
Interpret APGAR scores.
Discover problems of newborns
Heredity: The Epigenetic Framework
Nature or Nurture?
In this lesson, we will look at some of the ways in which heredity helps to shape the way we are. We will look at what happens genetically during conception and take a brief look some genetic abnormalities. Before going into these topics, however, it is important to emphasize the interplay between heredity and the environment. Why are you the way you are? As you consider some of your features (height, weight, personality, being diabetic, etc.), ask yourself whether these features are a result of heredity or environmental factors-or both. Chances are, you can see the ways in which both heredity and environmental factors (such as lifestyle, diet, and so on) have contributed to these features. For decades, scholars have carried on the “nature/nurture” debate. For any particular feature, those on the “nature” side would argue that heredity plays the most important role in bringing about that feature. Those on the “nurture” side would argue that one’s environment is most significant in shaping the way we are. This debate continues in questions about what makes us masculine or feminine (Lippa, 2002), concerns about vision (Mutti, Kadnik and Adams, 1996), and many other developmental issues. (Check out www.googlescholar.com for over 20,000 entries for “current nature/nurture debates”!) Yet most scholars agree that there is a constant interplay between the two forces. It is difficult to isolate the root of any single behavior as a result solely of nature or nurture and most scholars believe that even determining the extent to which nature or nurture impacts a human feature is difficult to answer. In fact, almost all human features are polygenic (a result of many genes) and multifactorial (a result of many factors, both genetic and environmental). It’s as if one’s genetic make-up sets up a range of possibilities, which may or may not be realized depending upon one’s environmental experiences. For instance, a person might be genetically predisposed to develop diabetes, but the person’s lifestyle may help bring about the disease.
The Epigenetic Framework
Gottlieb (1998, 2000, 2002) suggests an analytic framework for the nature/nurture debate that recognizes the interplay between the environment, behavior, and genetic expression. This bidirectional interplay suggests that the environment can effect the expression of genes just as genetic predispositions can impact a person’s potentials. And environmental circumstances can trigger symptoms of a genetic disorder. For example, a person who has sickle cell anemia, a recessive gene linked disorder, can experience a sickle cell crisis under conditions of oxygen deprivation. Someone predisposed genetically for type two diabetes can trigger the disease through poor diet and little exercise.
The Human Genome Project
The Human Genome Project is an internationally funded effort to map the locations of human genes and understand the role these genes play in development, health and illness. (Check out recent developments at www.genome.gov) Genes are segments of chromosomes (46 strands of a chemical substance called DNA that are contained in the nucleus of each normal human cell) that vary in length. There are an estimated 25,000 to 30,000 genes on each chromosome; a number far below the estimate of 100,000-150,000 held before the work of the Human Genome Project.
Understanding the role of genes in health and illness can bring about both harm and good (Weitz, 2007). A person who knows that they are at risk for developing a genetic disorder may be able to adopt lifestyle practices that minimize the risk and a person who discovers that they are not at risk may find comfort in knowing that they do not have to fear a particular disease. However, a person who finds out that they are at risk and there is nothing that can be done about it may experience years of fear and anxiety. And the availability of genetic testing may be more widespread than the availability of genetic counseling which can be very expensive. The possible stigma and discrimination that those with illness or at risk for illness must also be considered. In light of the high costs of health insurance, many companies are starting to offer benefits contingent on health assessments and lifestyle recommendations; and continued coverage depends on an employee following these recommendations. So a smoker may have to pay a higher premium than a non-smoker or a person who is overweight may be required to engage in a program of exercise and be monitored for improvement. What if a person finds out that they carry the gene for Huntington’s disease (a neurological disorder that is ultimately fatal) which may surface when a person reaches their 40s? The impact this knowledge will have on health care still remains unknown. Who should know what is on your genome? Do you think this information should be shared between mates? What about employers? What would be the advantages and disadvantages?
Conception
Gametes
There are two types of sex cells or gametes involved in reproduction: the male gametes or sperm and female gametes or ova. The male gametes are produced in the testes in a process called spermatogenesis which begin at about 12 years of age. The female gametes or ova which are stored in the ovaries are present at birth but are immature. Each ovary contains about 250,000 (Rome 1998) but only about 400 of these will become mature eggs (Mackon and Fauser 2000). Beginning at puberty, one ovum ripens and is released about every 28 days, a process called oogenesis.
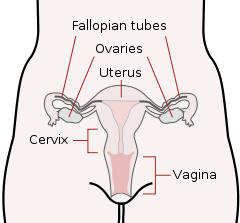
After the ovum or egg ripens and is released from the ovary, it is drawn into the fallopian tube and in 3 to 4 days, reaches the uterus. It is typically fertilized in the fallopian tube and continues its journey to the uterus. At ejaculation, millions of sperm are released into the vagina, but only a few reach the egg and typically, only one fertilizes the egg. Once a single sperm has entered the wall of the egg, the wall becomes hard and prevents other sperm from entering. After the sperm has entered the egg, the tail of the sperm breaks off and the head of the sperm, containing the genetic information from the father, unites with the nucleus of the egg. As a result, a new cell is formed. This cell, containing the combined genetic information from both parents, is referred to as a zygote.
Chromosomes contain genetic information from each parent. While other normal human cells have 46 chromosomes (or 23 pair), gametes contain 23 chromosomes. In a process called meiosis, segments of the chromosomes from each parent form pairs and genetic segments are exchanged as determined by chance. Because of the unpredictability of this exchange the likelihood of having offspring that are genetically identical (and not twins) is one in trillions (Gould and Keeton, 1997).
Determining the Sex of the Child
Twenty-two of those chromosomes from each parent are similar in length to a corresponding chromosome from the other parent. However, the remaining chromosome looks like an X or a Y. Half of the male’s sperm contain a Y chromosome and half contain an X. All of the ova contain two X chromosomes. If the child receives the combination of XY, the child will be genetically male. If it receives the XX combination, the child will be genetically female.
Many potential parents have a clear preference for having a boy or a girl and would like to determine the sex of the child. Through the years, a number of tips have been offered for the potential parents to maximize their chances for having either a son or daughter as they prefer. For example, it has been suggested that sperm which carry a Y chromosome are more fragile than those carrying an X. So, if a couple desires a male child, they can take measures to maximize the chance that the Y sperm reaches the egg. This involves having intercourse 48 hours after ovulation, which helps the Y sperm have a shorter journey to reach the egg, douching to create a more alkaline environment in the vagina, and having the female reach orgasm first so that sperm are not pushed out of the vagina during orgasm. Today, however, there is new technology available that makes it possible to isolate sperm containing either an X or a Y, depending on the preference, and use that sperm to fertilize a mother’s egg.
Monozygotic and Dizygotic Twins
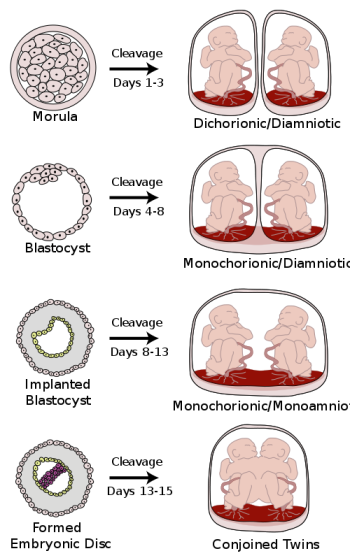
Monozygotic twins occur when a single zygote or fertilized egg splits apart in the first two weeks of development. The result is the creation of two separate but genetically identical offspring. About one-third of twins are monozygotic twins. Are you an identical twin?
Sometimes, however, two eggs or ova are released and fertilized by two separate sperm. The result is dizygotic or fraternal twins. About two-thirds of twins are dizygotic. These two individuals share the same amount of genetic material as would any two children from the same mother and father. Older mothers are more likely to have dizygotic twins than are younger mothers and couples who use fertility drugs are also more likely to give birth to dizygotic twins. Consequently, there has been in increase in the number of fraternal twins in recent years (Bortolus et. al., 1999).
What are the other possibilities? Various degrees of sharing the placenta can occur depending on the timing of the separation and duplication of cells. This is known as placentiation. Here is a diagram that illustrates various types of twins.
Author Kevin Dufenbach
Genotypes and Phenotypes (or why what you get is not always what you see)
The word genotype refers to the sum total of all the genes a person inherits. The word phenotype refers to the features that are actually expressed. Look in the mirror. What do you see, your genotype or your phenotype? What determines whether or not genes are expressed? Actually, this is quite complicated (Berger, 2005). Some features follow the additive pattern which means that many different genes contribute to a final outcome. Height and skin tone are examples. In other cases, a gene might either be turned on or off depending on the gene with which it is paired. Some genes are considered dominant because they will be expressed. Others, termed recessive, are only expressed in the absence of a dominant gene. Some characteristics which were once thought of as dominant-recessive, such as eye color, are now believed to be a result of the interaction between several genes (McKusick, 1998). Dominant traits include curly hair, facial dimples, normal vision, and dark hair. Recessive characteristics include red hair, pattern baldness, and nearsightedness. Sickle cell anemia is a recessive disease; Huntington disease is a dominant disease. Other traits are a result of partial dominance or co-dominance in which both genes are influential. For example, if a person inherits both recessive genes for sickle cell anemia, the disease will occur. But if a person has only one recessive gene for the disease, the person may experience effects of the disease only under circumstances of oxygen deprivation such as high altitudes or physical exertion (Berk, 2004).
Chromosomal Abnormalities and Genetic Disorders
A chromosomal abnormality occurs when there a child inherits too many or two few chromosomes. The most common cause of chromosomal abnormalities is the age of the mother. A 20 year old woman has a 1 in 800 chance of having a child with a common chromosomal abnormality. A woman of 44, however, has a one in 16 chance. It is believed that the problem occurs when the ovum is ripening prior to ovulation each month. As the mother ages, the ovum is more likely to suffer abnormalities at this time.
Some gametes do not divide evenly when they are forming. Therefore, some cells have more than 46 chromosomes. In fact, it is believed that close to half of all zygotes have an odd number of chromosomes. Most of these zygotes fail to develop and are spontaneously aborted by the body. If the abnormal number occurs on pair #21 or # 23, however, the individual may have certain physical or other abnormalities.
One of the most common chromosomal abnormalities is on pair 21. Trisomy 21 occurs when there are three rather than two chromosomes on #21. A person with Down syndrome experiences problems such as mental retardation and certain physical features such as having short fingers and toes, having folds of skin over the eyes, and a protruding tongue. Life expectancy of persons with Down syndrome has increased in recent years. Keep in mind that there is as much variation in people with Down Syndrome as in most populations and those differences need to be recognized and appreciated. Watch the following video clip about Down Syndrome from the National Down Syndrome Society:
When the abnormality is on pair #23, the result is a sex-linked chromosomal abnormality. A person might have XXY, XYY, XXX, XO, or 45 or 47 chromosomes as a result. Two of the more common sex-linked chromosomal disorders are Turner’s syndrome and Klinefelter’s syndrome. Turner’s syndrome occurs in 1 of every 2,500 live female births (Carroll, 2007) when an ovum which lacks a chromosome is fertilized by a sperm with an X chromosome. The resulting zygote has an XO composition. Fertilization by a Y sperm is not viable. Turner syndrome affects cognitive functioning and sexual maturation. The external genitalia appear normal, but breasts and ovaries do not develop fully and the woman does not menstruate. Turner’s syndrome also results in short stature and other physical characteristics. Learn more at www.turnersyndrome.org/. Klinefelter’s syndrome (XXY) occurs in 1 out of 700 live male births and results when an ovum containing an extra X chromosome is fertilized by a Y sperm. The Y chromosome stimulates the growth of male genitalia, but the additional X chromosome inhibits this development. An individual with Klinefelter’s syndrome has some breast development, infertility (this is the most common cause of infertility in males), and has low levels of testosterone.
Most of the known genetic disorders are dominant gene-linked; however, the vast majority of dominant gene linked disorders are not serious disorders, or if they are, they may still not be debilitating. For example, the majority of those with Tourette’s Syndrome suffer only minor tics from time to time and can easily control or cover up their symptoms. Huntington’s Disease is a dominant gene linked disorder that affects the nervous system and is fatal but does not appear until midlife. Recessive gene disorders, such as cystic fibrosis and sickel-cell anemia, are less common but may actually claim more lives because they are less likely to be detected as people are unaware that they are carriers of the disease. If the genes inherited from each parent are the same, the child is homozygous for a particular trait and will inherit the trait. If, however, the child inherits a gene from one parent but not the other, the child is heterozygous, and interaction between the genes will in part determine whether or not that trait is expressed (Berk, 2004).
REFERENCES
Berger, K. S. (2005). The developing person through the life span (6th ed.). New York: Worth.
Berk, L. (2004). Development through the life span (3rd ed.). Boston: Allyn and Bacon.
Bortolus, R., Parazzini, F., Chatenoud, L., Benzi, G., Bianchi, M. M., & Marini, A. (1999). The epidemiology of multiple births. Human Reproduction Update, 5, 179-187.
Brazelton, T. B., & Nugent, J. K. (1995). Neonatal behavioral assessment scale. London: Mac Keith Press.
Carrell, D. T., Wilcox, A. L., Lowry, L., Peterson, C. M., Jones, K. P., & Erikson, L. (2003). Elevated sperm chromosome aneuploidy and apoptosis in patients with unexplained recurrent pregnancy loss. Obstetrics and Gynecology, 101(6), 1229-1235.
Carroll, J. L. (2007). Sexuality now: Embracing diversity (2nd ed.). Belmont, CA: Thomson.
Dietrich, K. N. (1999). Environmental toxicants and child development. In Tager-Flusberg (Ed.), Neurodevelopmental disorders (pp. 469-490). Boston: MIT Press.
Galinsky, E. (1987). The six stages of parenthood. Reading, MA: Addison-Wesley Pub.
Gottlieb, G. (1998). Normally occurring environmental and behavioral influences on gene activity: From central dogma to probabilistic epigenesis. Psychological Review, 105, 792-802.
Gottlieb, G. (2000). Environmental and behavioral influences on gene activity. Current Directions in Psychological Science, 9, 93-97.
Gottlieb, G. (2002). Individual development and evolution: The genesis of novel behavior. New York: Oxford University Press.
Gould, J. L. (1997). Biological science. New York: Norton.
Lippa, R. A. (2002). Gender, nature, and nurture. Mahwah, NJ: L. Erlbaum.
MacDorman, M., Menacker, F., & Declercq, E. (2010, August 30). Trends and Characteristics of Home and Other out of Hospital Births in the United States, 1990-2006 (United States, Center for Disease Control). Retrieved December 22, 2010, from http://www.cdc.gov/nchs/data/nvsr/nv...;nvsr58_11.PDF
Mackon, N., & Fauser, B. (2000). Aspects of ovarian follicle development throughout life. Hormone Research, 52, 161-170.
McKusick, V. A. (1998). Mendelian inheritance in man: A catalog of human genes and genetic disorders. Baltimore, MD: Johns Hopkins University Press.
Moore, K. L., & Persaud, T. V. (1998). Before we are born (5th ed.). Philadelphia, PA: Saunders.
Mutti, D. O., Zadnik, K., & Adams, A. J. (n.d.). Myopia. The nature versus nurture debate goes on. Investigative Ophthalmology & Visual Science. Retrieved May 03, 2011, from http://www.iovs.org/cgi/reprint/37/6/952
Newell, M. (2005). Current issues in the prevention of mother-to-child transmission of HIV-1 infection. Transactions of the Royal Society of Tropical Medicine and Hygiene, 100(1), 1-5. doi: 10.1016/j.trstmh.2005.05.012
Rome, E. (1998). Anatomy and physiology of sexuality and reproduction. In The New Our Bodies, Ourselves (pp. 241-258). Carmichael, CA: Touchstone Books.
United States, Center for Disease Control. (n.d.). The Health Consequences of Smoking: 2004 Report of the Surgeon General. Retrieved August 14, 2004, from http://www.cdc.gov/tobacco/sqr/sqr_2004
United States, Center for Disease Control. (2006, July/August). Sexually Transmitted Diseases Treatment Guidelines. Retrieved August 14, 2006, from http://www.cdc.gov/std/treatment/2006/rr5511.pdf
United States, Center for Disease Control, Health and Human Services. (2010, October 5). Centers for Disease Control and Prevention. Retrieved May 03, 2011, from http://www.cdc.gov/nchs/faststats/birthwt.htm
United States, Center for Disease Control, National Center on Birth Defects and Developmental Disabilities. (2004, October 29). Fast Facts about Medication Use during Pregnancy and While Breastfeeding. Retrieved August 10, 2006, from http://www.cdc.gov/ncbddd/fas/fasask.htm