How did you come to be who you are? From beginning as a one-cell structure to your birth, your prenatal development occurred in an orderly and delicate sequence. There are three stages of prenatal development: germinal, embryonic, and fetal. Keep in mind that this is different than the three trimesters of pregnancy. Let’s take a look at what happens to the developing baby in each of these stages.
Prenatal Development
“The body of the unborn baby is more complex than ours. The preborn baby has several extra parts to his body which he needs only so long as he lives inside his mother. He has his own space capsule, the amniotic sac. He has his own lifeline, the umbilical cord, and he has his own root system, the placenta. These all belong to the baby himself, not to his mother. They are all developed from his original cell.”
Let’s take a look at some of the changes that take place during each of the three periods of prenatal development: the germinal period, the embryonic period, and the fetal period.
The Germinal Period (Weeks 1-2)

Figure 2. Sperm and Ovum at Conception
Conception occurs when a sperm fertilizes an egg and forms a zygote, which begins as a one-cell structure. The mother and father’s DNA is passed on to the child at the moment of conception. The genetic makeup and sex of the baby are set at this point. The germinal period (about 14 days in length) lasts from conception to implantation of the zygote (fertilized egg) in the lining of the uterus.
During the first week after conception, the zygote divides and multiplies, going from a one-cell structure to two cells, then four cells, then eight cells, and so on. The process of cell division is called mitosis. After the fourth division, differentiation of the cells begins to occur as well. Differentiated cells become more specialized, forming different organs and body parts. After 5 days of mitosis, there are 100 cells, and after 9 months there are billions of cells. Mitosis is a fragile process, and fewer than one-half of all zygotes survive beyond the first two weeks (Hall, 2004).
After the zygote divides for about 7–10 days and has 150 cells, it travels down the fallopian tubes and implants itself in the lining of the uterus. It’s estimated that about 60 percent of natural conceptions fail to implant in the uterus. The rate is higher for in vitro conceptions. Once the zygote attaches to the uterus, the next stage begins.
The Embryonic Period (Weeks 3-8)

Figure 3. Human Embryo
The embryonic period begins once the zygote is implanted in the uterine wall. It lasts from the third through the eighth week after conception. Upon implantation, this multi-cellular organism is called an embryo. Now blood vessels grow, forming the placenta. The placenta is a structure connected to the uterus that provides nourishment and oxygen from the mother to the developing embryo via the umbilical cord.
During this period, cells continue to differentiate. Basic structures of the embryo start to develop into areas that will become the head, chest, and abdomen. During the embryonic stage, the heart begins to beat and organs form and begin to function. At 22 days after conception, the neural tube forms along the back of the embryo, developing into the spinal cord and brain.
Growth during prenatal development occurs in two major directions: from head to tail (cephalocaudal development) and from the midline outward (proximodistal development). This means that those structures nearest the head develop before those nearest the feet and those structures nearest the torso develop before those away from the center of the body (such as hands and fingers).
The head develops in the fourth week and the precursor to the heart begins to pulse. In the early stages of the embryonic period, gills and a tail are apparent. But by the end of this stage, they disappear and the organism takes on a more human appearance. The embryo is approximately 1 inch in length and weighs about 4 grams at the end of this period. The embryo can move and respond to touch at this time.
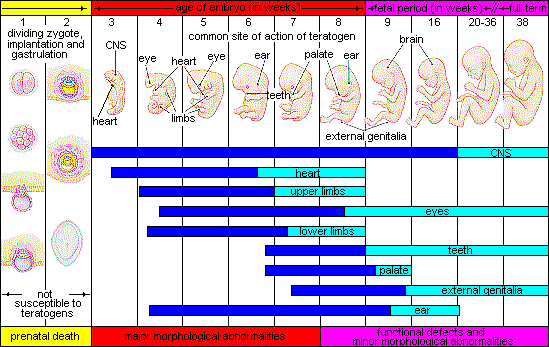
About 20 percent of organisms fail during the embryonic period, usually due to gross chromosomal abnormalities. As in the case of the germinal period, often the mother does not yet know that she is pregnant. It is during this stage that the major structures of the body are taking form making the embryonic period the time when the organism is most vulnerable to the greatest amount of damage if exposed to harmful substances. Potential mothers are not often aware of the risks they introduce to the developing child during this time.
The Fetal Period (Weeks 9-40)

Figure 4. A fetus at 10 weeks of development.
When the organism is about nine weeks old, the embryo is called a fetus. At this stage, the fetus is about the size of a kidney bean and begins to take on the recognizable form of a human being as the “tail” begins to disappear.
From 9–12 weeks, the sex organs begin to differentiate. By the 12th week, the fetus has all its body parts including external genitalia. In the following weeks, the fetus will develop hair, nails, teeth and the excretory and digestive systems will continue to develop. At the end of the 12th week, the fetus is about 3 inches long and weighs about 28 grams.
At about 16 weeks, the fetus is approximately 4.5 inches long. Fingers and toes are fully developed, and fingerprints are visible. During the 4-6th months, the eyes become more sensitive to light and hearing develops. The respiratory system continues to develop. Reflexes such as sucking, swallowing, and hiccuping develop during the 5th month. Cycles of sleep and wakefulness are present at that time as well. Throughout the fetal stage, the brain continues to grow and develop, nearly doubling in size from weeks 16 to 28. The majority of the neurons in the brain have developed by 24 weeks although they are still rudimentary and the glial or nurse cells that support neurons continue to grow. At 24 weeks the fetus can feel pain (Royal College of Obstetricians and Gynecologists, 1997).
The first chance of survival outside the womb, known as the age of viability is reached at about 22 to 26 weeks (Moore & Persaud, 1998). By the time the fetus reaches the sixth month of development (24 weeks), it weighs up to 1.4 pounds. The hearing has developed, so the fetus can respond to sounds. The internal organs, such as the lungs, heart, stomach, and intestines, have formed enough that a fetus born prematurely at this point has a chance to survive outside of the mother’s womb.
Between the 7th and 9th months, the fetus is primarily preparing for birth. It is exercising its muscles, its lungs begin to expand and contract. It is developing fat layers under the skin. The fetus gains about 5 pounds and 7 inches during this last trimester of pregnancy which includes a layer of fat gained during the 8th month. This layer of fat serves as insulation and helps the baby regulate body temperature after birth.
Around 36 weeks, the fetus is almost ready for birth. It weighs about 6 pounds and is about 18.5 inches long, and by week 37 all of the fetus’s organ systems are developed enough that it could survive outside the mother’s uterus without many of the risks associated with premature birth. The fetus continues to gain weight and grow in length until approximately 40 weeks. By then, the fetus has very little room to move around and birth becomes imminent.

Figure 5. During the fetal stage, the baby’s brain develops and the body adds size and weight until the fetus reaches full-term development.
This video on prenatal development explains many of the developmental milestones and changes that happen during each month of development for the embryo and fetus.
Complications of Pregnancy and Delivery

Figure 8. Pregnancy affects women in different ways; some notice few adverse side effects, while others feel high levels of discomfort, or develop more serious complications.
There are a number of common side effects of pregnancy. Not everyone experiences all of these nor do women experience them to the same degree. And although they are considered “minor” these problems are potentially very uncomfortable. These side effects include nausea (particularly during the first 3-4 months of pregnancy as a result of higher levels of estrogen in the system), heartburn, gas, hemorrhoids, backache, leg cramps, insomnia, constipation, shortness of breath or varicose veins (as a result of carrying a heavy load on the abdomen). What is the cure? Delivery!
Major Complications
The following are some serious complications of pregnancy which can pose health risks to mother and child and that often require special care.
- Gestational diabetes is when a woman without diabetes develops high blood sugar levels during pregnancy.
- Hyperemesis gravidarum is the presence of severe and persistent vomiting, causing dehydration and weight loss. It is more severe than the more common morning sickness.
- Preeclampsia is gestational hypertension. Severe preeclampsia involves blood pressure over 160/110 with additional signs. Eclampsia is seizures in a pre-eclamptic patient.
-
Deep vein thrombosis is the formation of a blood clot in a deep vein, most commonly in the legs.
- A pregnant woman is more susceptible to infections. This increased risk is caused by an increased immune tolerance in pregnancy to prevent an immune reaction against the fetus.
- Peripartum cardiomyopathy is a decrease in heart function which occurs in the last month of pregnancy, or up to six months post-pregnancy.
Maternal Mortality
Maternal mortality is unacceptably high. About 830 women die from pregnancy or childbirth-related complications around the world every day. It was estimated that in 2015, roughly 303,000 women died during and following pregnancy and childbirth. Almost all of these deaths occurred in low-resource settings, and most could have been prevented. The high number of maternal deaths in some areas of the world reflects inequities in access to health services and highlights the gap between rich and poor. Almost all maternal deaths (99%) occur in developing countries. More than half of these deaths occur in sub-Saharan Africa and almost one third occur in South Asia.
Almost all maternal deaths can be prevented, as evidenced by the huge disparities found between the richest and poorest countries. The lifetime risk of maternal death in high-income countries is 1 in 3,300, compared to 1 in 41 in low-income.
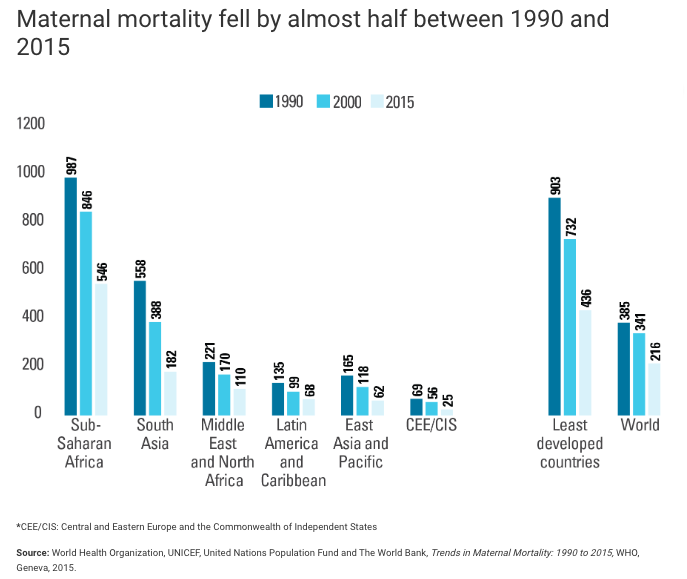
Figure 9. This graph shows declining maternal mortality rates, as measured as the number of deaths per 100,000 live births. in 1990, 903 out of 100,000 live births resulted in death in the least developed countries, but that number has improved to 436 out of 100,000 births in 2015. Globally, there were 216 deaths for every 100,000 live births in 2015. (Image Source:
UNICEF.)
Even though maternal mortality in the United States is relatively rare today because of advanced in medical care, it is still an issue that needs to be addressed. The number of reported pregnancy-related deaths in the United States steadily increased from 7.2 deaths per 100,000 live births in 1987 to 18.0 deaths per 100,000 live births in 2014. The Centers for Disease Control and Prevention define a pregnancy-related death as the death of a woman while pregnant or within 1 year of the end of a pregnancy–regardless of the outcome, duration, or site of the pregnancy–from any cause related to or aggravated by the pregnancy or its management, but not from accidental or incidental causes. The reasons for the overall increase in pregnancy-related mortality are unclear. What do you think are some reasons for this surprising increase in the United States? What can be done to change this statistic?
In the United States, black women are disproportionately more likely to die from complications related to pregnancy or childbirth than any other race; they are three or four times more likely than white women to die due to pregnancy-related death and are more likely to receive worse maternal care. Black women from higher income groups and with advanced education levels also have heightened risks—even tennis superstar Serena Williams had near-deadly complications during the birth of her daughter, Olympia. Why is this the case in our modern world? Watch this video to learn more:
An interactive or media element has been excluded from this version of the text. You can view it online here: https://iastate.pressbooks.pub/parentingfamilydiversity/?p=1681
The data below shows percentages of the causes of pregnancy-related deaths in the United States during 2011–2014:
-
Cardiovascular diseases, 15.2%.
-
Non-cardiovascular diseases, 14.7%.
-
Infection or sepsis, 12.8%.
-
Hemorrhage, 11.5%.
-
Cardiomyopathy, 10.3%.
-
Thrombotic pulmonary embolism, 9.1%.
-
Cerebrovascular accidents, 7.4%.
-
Hypertensive disorders of pregnancy, 6.8%.
-
Amniotic fluid embolism, 5.5%.
-
Anesthesia complications, 0.3%.
The cause of death is unknown for 6.5% of all 2011–2014 pregnancy-related deaths.
Miscarriage
Spontaneous abortion, or miscarriage, is experienced in an estimated 20-40 percent of undiagnosed pregnancies and in another 10 percent of diagnosed pregnancies. Usually, the body aborts due to chromosomal abnormalities and this typically happens before the 12th week of pregnancy. Cramping and bleeding result and normal periods return after several months. Some women are more likely to have repeated miscarriages due to chromosomal, amniotic, or hormonal problems; but miscarriage can also be a result of defective sperm (Carroll et al., 2003).