Middle and late childhood spans the ages between early childhood and adolescence, approximately ages 6 to 11 years. Children gain greater control over the movement of their bodies, mastering many gross and fine motor skills that eluded the younger child. Changes in the brain during this age enable not only physical development, but contributes to greater reasoning and flexibility of thought. School becomes a big part of middle and late childhood, and it expands their world beyond the boundaries of their own family. Peers start to take center-stage, often prompting changes in the parent-child relationship. Peer acceptance also influences children’s perception of self and may have consequences for emotional development beyond these years.
Rates of growth generally slow during these years. Typically, a child will gain about 5-7 pounds a year and grow about 2-3 inches per year. They also tend to slim down and gain muscle strength and lung capacity making it possible to engage in strenuous physical activity for long periods of time. The beginning of the growth spurt, which occurs prior to puberty, begins two years earlier for females than males. The mean age for the beginning of the growth spurt for girls is nine, while for boys it is eleven. Children of this age tend to sharpen their abilities to perform both gross motor skills, such as riding a bike, and fine motor skills, such as cutting their fingernails. In gross motor skills (involving large muscles) boys typically outperform girls, while with fine motor skills (small muscles) girls outperform the boys. These improvements in motor skills are related to brain growth and experience during this developmental period.
Two major brain growth spurts occur during middle/late childhood. Between ages 6 and 8, significant improvements in fine motor skills and eye-hand coordination are noted. Then between 10 and 12 years of age, the frontal lobes become more developed and improvements in logic, planning, and memory are evident. Children in middle to late childhood are also better able to plan, coordinate activity using both left and right hemispheres of the brain, and to control emotional outbursts. Paying attention is also improved as the prefrontal cortex matures.
Childhood Obesity
The decreased participation in school physical education and youth sports is just one of many factors that has led to an increase in children being overweight or obese. The current measurement for determining excess weight is the Body Mass Index (BMI) which expresses the relationship of height to weight. According to the Centers for Disease Control and Prevention (CDC), children’s whose BMI is at or above the 85th percentile for their age are considered overweight, while children who are at or above the 95th percentile are considered obese. Excess weight and obesity in children are associated with a variety of medical and cognitive conditions including high blood pressure, insulin resistance, inflammation, depression, and lower academic achievement.
Being overweight has also been linked to impaired brain functioning, which includes deficits in executive functioning, working memory, mental flexibility, and decision making. Children who ate more saturated fats performed worse on relational memory tasks while eating a diet high in omega-3 fatty acids promoted relational memory skills. Using animal studies Davidson et al. (2013) found that large amounts of processed sugars and saturated fat weakened the blood-brain barrier, especially in the hippocampus. This can make the brain more vulnerable to harmful substances that can impair its functioning. Another important executive functioning skill is controlling impulses and delaying gratification. Children who are overweight show less inhibitory control than normal-weight children, which may make it more difficult for them to avoid unhealthy foods. Overall, being overweight as a child increases the risk for cognitive decline as one ages.
A growing concern is the lack of recognition from parents that children are overweight or obese. Katz (2015) referred to this as “Oblivobesity”. Black et al. (2015) found that parents in the United Kingdom (UK) only recognized their children as obese when they were above the 99.7th percentile while the official cut-off for obesity is at the 85th percentile.[/footnote] Oude Luttikhuis, Stolk, and Sauer (2010) surveyed 439 parents and found that 75% of parents of overweight children said the child had a normal weight and 50% of parents of obese children said the child had a normal weight. For these parents, overweight was considered normal and obesity was considered normal or a little heavy. Doolen, Alpert, and Miller (2009) reported on several studies from the United Kingdom, Australia, Italy, and the United States, and in all locations parents were more likely to misperceive their children’s weight. Black, Park, and Gregson (2015) concluded that as the average weight of children rises, what parents consider normal also rises. Needless to say, if parents cannot identify if their children are overweight they will not be able to intervene and assist their children with proper weight management.
An added concern is that the children themselves are not accurately identifying if they are overweight. In a United States sample of 8-15 year-olds, more than 80% of overweight boys and 70% of overweight girls misperceived their weight as normal. Also noted was that as the socioeconomic status of the children rose, the frequency of these misconceptions decreased. It appeared that families with more resources were more conscious of what defines a healthy weight.
Children who are overweight tend to be rejected, ridiculed, teased and bullied by others more than their peer counterparts (Stopbullying.gov). This can certainly be damaging to their self-image and popularity. In addition, children who are obese run the risk of suffering orthopedic problems such as knee injuries, and they have an increased risk of heart disease and stroke in adulthood. It is hard for a child who is obese to become a non-obese adult. In addition, the number of cases of pediatric diabetes has risen dramatically in recent years.
Behavioral interventions, including training children to overcome impulsive behavior, are being researched to help children achieve and maintain a healthy weight. Practicing inhibition has been shown to strengthen the ability to resist unhealthy foods. Parents can help their children the best when they are warm and supportive without using shame or guilt. Parents can also act like the child’s frontal lobe until it is developed by helping them make correct food choices and praising their efforts. Research also shows that exercise, especially aerobic exercise, can help improve cognitive functioning in children. Parents should take caution against emphasizing diet alone to avoid the development of any obsession about dieting that can lead to eating disorders. Instead, increasing a child’s activity level is most helpful.
Recall from earlier chapters that children in early childhood are in Piaget’s preoperational stage, and during this stage, children are learning to think symbolically about the world. Cognitive skills continue to expand in middle and late childhood as thought processes become more logical and organized when dealing with concrete information. Children at this age understand concepts such as past, present, and future, giving them the ability to plan and work toward goals. Additionally, they can process complex ideas such as addition and subtraction and cause-and-effect relationships.
Concrete Operational Thought
From ages 7 to 11, children are in what Piaget referred to as the Concrete Operational Stage of cognitive development.This involves mastering the use of logic in concrete ways. The word concrete refers to that which is tangible; that which can be seen, touched, or experienced directly. The concrete operational child is able to make use of logical principles in solving problems involving the physical world. For example, the child can understand the principles of cause and effect, size, and distance.
The child can use logic to solve problems tied to their own direct experience, but has trouble solving hypothetical problems or considering more abstract problems. The child uses Inductive Reasoning, which is a logical process in which multiple premises believed to be true are combined to obtain a specific conclusion. For example, a child has one friend who is rude, another friend who is also rude, and the same is true for a third friend. The child may conclude that friends are rude. We will see that this way of thinking tends to change during adolescence being replaced with deductive reasoning. We will now explore some of the major abilities that the concrete child exhibits.
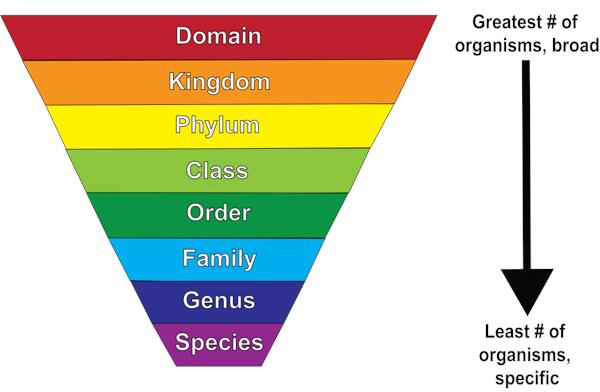
Figure 2. Children in the concrete operational stage understand how to classify organisms
- Classification: As children’s experiences and vocabularies grow, they build schemata and are able to organize objects in many different ways. They also understand classification hierarchies and can arrange objects into a variety of classes and subclasses.
- Identity: One feature of concrete operational thought is the understanding that objects have qualities that do not change even if the object is altered in some way. For instance, mass of an object does not change by rearranging it. A piece of chalk is still chalk even when the piece is broken in two.
- Reversibility: The child learns that some things that have been changed can be returned to their original state. Water can be frozen and then thawed to become liquid again. But eggs cannot be unscrambled. Arithmetic operations are reversible as well: 2 + 3 = 5 and 5 – 3 = 2.
Many of these cognitive skills are incorporated into the school’s curriculum through mathematical problems and in worksheets about which situations are reversible or irreversible.
- Conservation: Remember the example in our last chapter of preoperational children thinking that a tall beaker filled with 8 ounces of water was “more” than a short, wide bowl filled with 8 ounces of water? Concrete operational children can understand the concept of conservation which means that changing one quality (in this example, height or water level) can be compensated for by changes in another quality (width). Consequently, there is the same amount of water in each container, although one is taller and narrower and the other is shorter and wider.
- Decentration: Concrete operational children no longer focus on only one dimension of any object (such as the height of the glass) and instead consider the changes in other dimensions too (such as the width of the glass). This allows for conservation to occur.
- Seriation: Arranging items along a quantitative dimension, such as length or weight, in a methodical way is now demonstrated by the concrete operational child. For example, they can methodically arrange a series of different-sized sticks in order by length, while younger children approach a similar task in a haphazard way.
These new cognitive skills increase the child’s understanding of the physical world, however according to Piaget, they still cannot think in abstract ways. Additionally, they do not think in systematic scientific ways. For example, when asked which variables influence the period that a pendulum takes to complete its arc, and given weights they can attach to strings in order to do experiments, most children younger than 12 perform biased experiments from which no conclusions can be drawn.
Intellectual Disability and Giftedness
The results of studies assessing the measurement of intelligence show that IQ is distributed in the population in the form of a Normal Distribution (or bell curve), which is the pattern of scores usually observed in a variable that clusters around its average. In a normal distribution, the bulk of the scores fall toward the middle, with many fewer scores falling at the extremes. The normal distribution of intelligence shows that on IQ tests, as well as on most other measures, the majority of people cluster around the average (in this case, where IQ = 100), and fewer are either very smart or very dull (see Figure 5.13). Because the standard deviation of an IQ test is about 15, this means that about 2% of people score above an IQ of 130, often considered the threshold for giftedness, and about the same percentage score below an IQ of 70, often being considered the threshold for an intellectual disability.
Although Figure 5.13 presents a single distribution, the actual IQ distribution varies by sex such that the distribution for men is more spread out than is the distribution for women. These sex differences mean that about 20% more men than women fall in the extreme (very smart or very dull) ends of the distribution. Boys are about five times more likely to be diagnosed with the reading disability dyslexia than are girls, and are also more likely to be classified as having an intellectual disability. However, boys are also about 20% more highly represented in the upper end of the IQ distribution.
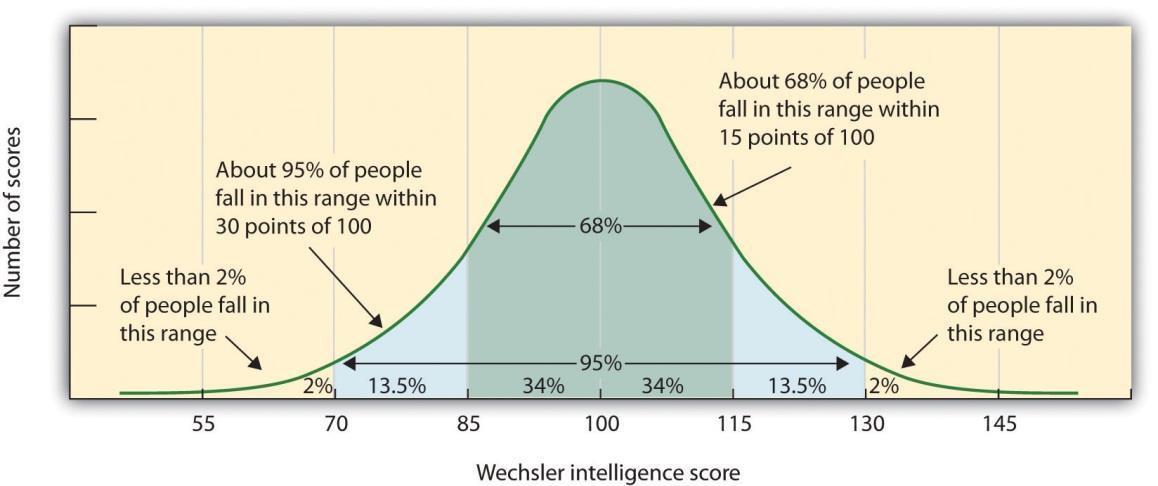
Figure 3. Distribution of IQ Scores in the General PopulationThe normal distribution of IQ scores in the general population shows that most people have about average intelligence, while very few have extremely high or extremely low intelligence.
One end of the distribution of intelligence scores is defined by people with very low IQ. Intellectual disability (or intellectual developmental disorder) is assessed based on cognitive capacity (IQ) and adaptive functioning. The severity of the disability is based on adaptive functioning, or how well the person handles everyday life tasks. About 1% of the United States population, most of them males, fulfill the criteria for intellectual developmental disorder, but some children who are given this diagnosis lose the classification as they get older and better learn to function in society. A particular vulnerability of people who have a low IQ is that they may be taken advantage of by others, and this is an important aspect of the definition of intellectual developmental disorder.
One cause of intellectual developmental disorder is Down syndrome, a chromosomal disorder caused by the presence of all or part of an extra 21st chromosome. The incidence of Down syndrome is estimated at approximately 1 per 700 births, and the prevalence increases as the mother’s age increases. People with Down syndrome typically exhibit a distinctive pattern of physical features, including a flat nose, upwardly slanted eyes, a protruding tongue, and a short neck.
Fortunately, societal attitudes toward individuals with intellectual disabilities have changed over the past decades. We no longer use terms such as “retarded,” “moron,” “idiot,” or “imbecile” to describe people with intellectual deficits, although these were the official psychological terms used to describe degrees of what was referred to as mental retardation in the past. Laws such as the Americans with Disabilities Act (ADA) have made it illegal to discriminate on the basis of mental and physical disability, and there has been a trend to bring people with mental disabilities out of institutions and into our workplaces and schools.
Giftedness refers to children who have an IQ of 130 or higher. Having extremely high IQ is clearly less of a problem than having extremely low IQ, but there may also be challenges to being particularly smart. It is often assumed that schoolchildren who are labeled as “gifted” may have adjustment problems that make it more difficult for them to create social relationships. To study gifted children, Lewis Terman and his colleagues selected about 1,500 high school students who scored in the top 1% on the Stanford-Binet and similar IQ tests (i.e., who had IQs of about 135 or higher), and tracked them for more than seven decades (the children became known as the “termites” and are still being studied today). This study found that these students were not unhealthy or poorly adjusted, but rather were above average in physical health and were taller and heavier than individuals in the general population. The students also had above-average social relationships and were less likely to divorce than the average person.
Terman’s study also found that many of these students went on to achieve high levels of education and entered prestigious professions, including medicine, law, and science. Of the sample, 7% earned doctoral degrees, 4% earned medical degrees, and 6% earned law degrees. These numbers are all considerably higher than what would have been expected from a more general population. Another study of young adolescents who had even higher IQs found that these students ended up attending graduate school at a rate more than 50 times higher than that in the general population.
As you might expect based on our discussion of intelligence, kids who are gifted have higher scores on general intelligence “g”, but there are also different types of giftedness. Some children are particularly good at math or science, some at automobile repair or carpentry, some at music or art, some at sports or leadership, and so on. There is a lively debate among scholars about whether it is appropriate or beneficial to label some children as “gifted and talented” in school and to provide them with accelerated special classes and other programs that are not available to everyone. Although doing so may help the gifted kids, it also may isolate them from their peers and make such provisions unavailable to those who are not classified as “gifted.”
Education
Remember the ecological systems model that we explored? This model helps us understand an individual by examining the contexts in which the person lives and the direct and indirect influences on that person’s life. School becomes a very important component of children’s lives during middle and late childhood, and parents and the culture contribute to children’s experiences in school as indicated by the ecological systems model through their interaction with the school.
Parental Involvement in School
Parents vary in their level of involvement with their children’s schools. Teachers often complain that they have difficulty getting parents to participate in their child’s education and devise a variety of techniques to keep parents in touch with daily and overall progress. For example, parents may be required to sign a behavior chart each evening to be returned to school or may be given information about the school’s events through websites and newsletters. There are other factors that need to be considered when looking at parental involvement. To explore these, first ask yourself if all parents who enter the school with concerns about their child be received in the same way?
Horvat (2004) found that teachers seek a particular type of involvement from particular types of parents. While teachers thought they were open and neutral in their responses to parental involvement, in reality teachers were most receptive to support, praise and agreement coming from parents who were most similar in race and social class with the teachers. Parents who criticized the school or its policies were less likely to be given voice. Parents who have higher levels of income, occupational status, and other qualities favored in society have family capital. This is a form of power that can be used to improve a child’s education. Parents who do not have these qualities may find it more difficult to be effectively involved. The authors suggest that teachers closely examine their biases. Schools may also need to examine their ability to dialogue with parents about school policies in more open ways. Any efforts to improve effective parental involvement should address these concerns.
Children with Disabilities
A Learning Disability (or LD) is a specific impairment of academic learning that interferes with a specific aspect of schoolwork and that reduces a student’s academic performance significantly. An LD shows itself as a major discrepancy between a student’s ability and some feature of achievement: The student may be delayed in reading, writing, listening, speaking, or doing mathematics, but not in all of these at once. A learning problem is not considered a learning disability if it stems from physical, sensory, or motor handicaps, or from generalized intellectual impairment. It is also not an LD if the learning problem really reflects the challenges of learning English as a second language. Genuine LDs are the learning problems left over after these other possibilities are accounted for or excluded. Typically, a student with an LD has not been helped by teachers’ ordinary efforts to assist the student when he or she falls behind academically, though what counts as an “ordinary effort”, of course, differs among teachers, schools, and students. Most importantly, though, an LD relates to a fairly specific area of academic learning. A student may be able to read and compute well enough, for example, but not be able to write. LDs are by far the most common form of special educational need, accounting for half of all students with special needs in the United States and anywhere from 5 to 20 percent of all students, depending on how the numbers are estimated., Students with LDs are so common, in fact, that most teachers regularly encounter at least one per class in any given school year, regardless of the grade level they teach.
These difficulties are identified in school because this is when children’s academic abilities are being tested, compared, and measured. Consequently, once academic testing is no longer essential in that person’s life (as when they are working rather than going to school) these disabilities may no longer be noticed or relevant, depending on the person’s job and the extent of the disability.
Dyslexia is one of the most commonly diagnosed disabilities and involves having difficulty in the area of reading. This diagnosis is used for a number of reading difficulties. Common characteristics are difficulty with phonological processing, which includes the manipulation of sounds, spelling, and rapid visual/verbal processing. Additionally, the child may reverse letters, have difficulty reading from left to right, or may have problems associating letters with sounds. It appears to be rooted in neurological problems involving the parts of the brain active in recognizing letters, verbally responding, or being able to manipulate sounds. Recent studies have identified a number of genes that are linked to developing dyslexia. Treatment typically involves altering teaching methods to accommodate the person’s particular problematic area.
ADHD
Figure 4. Some adolescents find it difficult to concentrate on complex tasks due to ADHD.
A child with Attention Deficit Hyperactivity Disorder (ADHD) shows a constant pattern of inattention and/or hyperactive and impulsive behavior that interferes with normal functioning. Some of the signs of inattention include great difficulty with, and avoidance of, tasks that require sustained attention (such as conversations or reading), failure to follow instructions (often resulting in failure to complete schoolwork and other duties), disorganization (difficulty keeping things in order, poor time management, sloppy and messy work), lack of attention to detail, becoming easily distracted, and forgetfulness. Hyperactivity is characterized by excessive movement, and includes fidgeting or squirming, leaving one’s seat in situations when remaining seated is expected, having trouble sitting still (e.g., in a restaurant), running about and climbing on things, blurting out responses before another person’s question or statement has been completed, difficulty waiting for one’s turn for something, and interrupting and intruding on others. Frequently, the hyperactive child comes across as noisy and boisterous. The child’s behavior is hasty, impulsive, and seems to occur without much forethought; these characteristics may explain why adolescents and young adults diagnosed with ADHD receive more traffic tickets and have more automobile accidents than do others their age.

Figure 5. Children may be hyperactive or exceptionally quiet when exhibiting signs of ADHD. Symptoms tend to display differently in girls.
ADHD occurs in about 5% of children. On average, boys are 3 times more likely to have ADHD than are girls; however, such findings might reflect the greater propensity of boys to engage in aggressive and antisocial behavior and thus incur a greater likelihood of being referred to psychological clinics. Children with ADHD face severe academic and social challenges. Compared to their non-ADHD counterparts, children with ADHD have lower grades and standardized test scores and higher rates of expulsion, grade retention, and dropping out. They also are less well-liked and more often rejected by their peers.
ADHD can persist into adolescence and adulthood. A recent study found that 29.3% of adults who had been diagnosed with ADHD decades earlier still showed symptoms. Somewhat troubling, this study also reported that nearly 81% of those whose ADHD persisted into adulthood had experienced at least one other comorbid disorder, compared to 47% of those whose ADHD did not persist. Additional concerns when an adult has ADHD include Worse educational attainment, lower socioeconomic status, less likely to be employed, more likely to be divorced, and more likely to have non-alcohol-related substance abuse problems.
Causes of ADHD
Family and twin studies indicate that genetics play a significant role in the development of ADHD. Burt (2009), in a review of 26 studies, reported that the median rate of concordance for identical twins was .66, whereas the median concordance rate for fraternal twins was .20. The specific genes involved in ADHD are thought to include at least two that are important in the regulation of the neurotransmitter dopamine, suggesting that dopamine may be important in ADHD. Indeed, medications used in the treatment of ADHD, such as methylphenidate (Ritalin) and amphetamine with dextroamphetamine (Adderall), have stimulant qualities and elevate dopamine activity. People with ADHD show less dopamine activity in key regions of the brain, especially those associated with motivation and reward, which provides support to the theory that dopamine deficits may be a vital factor in the development of this disorder.
Brain imaging studies have shown that children with ADHD exhibit abnormalities in their frontal lobes, an area in which dopamine is in abundance. Compared to children without ADHD, those with ADHD appear to have smaller frontal lobe volume, and they show less frontal lobe activation when performing mental tasks. Recall that one of the functions of the frontal lobes is to inhibit our behavior. Thus, abnormalities in this region may go a long way toward explaining the hyperactive, uncontrolled behavior of ADHD.
Although some food additives have been shown to increase hyperactivity in non-ADHD children, the effect is rather small. Numerous studies, however, have shown a significant relationship between exposure to nicotine in cigarette smoke during the prenatal period and ADHD. Maternal smoking during pregnancy is associated with the development of more severe symptoms of the disorder.
Treatment for ADHD
Recommended treatment for ADHD includes behavioral interventions, cognitive behavioral therapy, parent and teacher education, recreational programs, and lifestyle changes, such as getting more sleep. For some children medication is prescribed. Parents are often concerned that stimulant medication may result in their child acquiring a substance use disorder. However, research using longitudinal studies has demonstrated that children diagnosed with ADHD who received pharmacological treatment had a lower risk for substance abuse problems than those children who did not receive medication.
Is the prevalence rate of ADHD increasing?
Many people believe that the rates of ADHD have increased in recent years, and there is evidence to support this contention. ADHD may be over-diagnosed by doctors who are too quick to medicate children as a behavior treatment. There is also greater awareness of ADHD now than in the past. Nearly everyone has heard of ADHD, and most parents and teachers are aware of its key symptoms. Thus, parents may be quick to take their children to a doctor if they believe their child possesses these symptoms, or teachers may be more likely now than in the past to notice the symptoms and refer the child for evaluation. Further, the use of computers, video games, iPhones, and other electronic devices has become pervasive among children in the early 21st century, and these devices could potentially shorten children’s attention spans. Thus, what might seem like inattention to some parents and teachers could simply reflect exposure to too much technology.
Legislation for Learning Disabilities
Since the 1970s political and social attitudes have moved increasingly toward including people with disabilities into a wide variety of “regular” activities. In the United States, the shift is illustrated clearly in the Federal legislation that was enacted during this time. Three major laws were passed that guaranteed the rights of persons with disabilities, and of children and students with disabilities in particular. The third law has had the biggest impact on education.
Rehabilitation Act of 1973, Section 504
This law, the first of its kind, required that individuals with disabilities be accommodated in any program or activity that receives Federal funding. Although this law was not intended specifically for education, in practice it has protected students’ rights in some extra-curricular activities (for older students) and in some child care or after-school care programs (for younger students). If those programs receive Federal funding of any kind, the programs are not allowed to exclude children or youths with disabilities, and they have to find reasonable ways to accommodate the individuals’ disabilities.
Americans with Disabilities Act of 1990 (or ADA)
This legislation also prohibited discrimination on the basis of disability, just as Section 504 of the Rehabilitation Act had done. Although the ADA also applies to all people (not just to students), its provisions are more specific and “stronger” than those of Section 504. In particular, ADA extends to all employment and jobs, not just those receiving Federal funding. It also specifically requires accommodations to be made in public facilities such as with buses, restrooms, and telephones. ADA legislation is therefore responsible for some of the “minor” renovations in schools that you may have noticed in recent years, like wheelchair-accessible doors, ramps, and restrooms, and public telephones with volume controls.
Individuals with Disabilities Education Act (or IDEA)
As its name implied this legislation was more focused on education than either Section 504 or ADA. It was first passed in 1975 and has been amended several times since, including most recently in 2004. In its current form, the law guarantees the following rights related to education for anyone with a disability from birth to age 21. The first two influence schooling in general, but the last three affect the work of classroom teachers rather directly:
- Free, appropriate education: An individual or an individual’s family should not have to pay for education simply because the individual has a disability, and the educational program should be truly educational; i.e., not merely care-taking or babysitting the person.
- Due process: In case of disagreements between an individual with a disability and the schools or other professionals, there must be procedures for resolving the disagreements that are fair and accessible to all parties, including the person himself or herself or the person’s representative.
- Fair evaluation of performance in spite of disability: Tests or other evaluations should not assume test-taking skills that a person with a disability cannot reasonably be expected to have, such as holding a pencil, hearing or seeing questions, working quickly, or understanding and speaking orally. Evaluation procedures should be modified to allow for these differences. This provision of the law applies both to evaluations made by teachers and to school-wide or “high-stakes” testing programs.
- Education in the “least restrictive environment”: Education for someone with a disability should provide as many educational opportunities and options for the person as possible, both in the short term and in the long term. In practice, this requirement has meant including students in regular classrooms and school activities as much as possible, though often not totally.
- An individualized educational program: Given that every disability is unique, instructional planning for a person with a disability should be unique or individualized as well. In practice, this provision has led to classroom teachers planning individualized programs jointly with other professionals (like reading specialists, psychologists, or medical personnel) as part of a team.
Evaluation and diagnosis can be the first step in helping provide children with disabilities the type of instruction and resources that will benefit them educationally, but diagnosis and labeling also have social implications. It is important to consider that children can be misdiagnosed and that once a child has received a diagnostic label, the child, teachers, and family members may tend to interpret actions of the child through that label. The label can also influence the child’s self-concept. Consider, for example, a child who is misdiagnosed as learning disabled. That child may expect to have difficulties in school, lack confidence, and because of these expectations experience trouble. This self-fulfilling prophecy calls our attention to the power that labels can have whether or not they are accurately applied. It is also important to consider that children’s difficulties can change over time; a child who has problems in school may improve later or may live under circumstances as an adult where the problem (such as a delay in math skills or reading skills) is no longer relevant. That person, however, will still have a label as learning disabled. It should be recognized that the distinction between abnormal and normal behavior is not always clear; some abnormal behavior in children is fairly common.
Erikson: Industry vs. Inferiority
According to Erikson, children in middle and late childhood are very busy or industrious. They are constantly doing, planning, playing, getting together with friends, and achieving. This is a very active time, and a time when they are gaining a sense of how they measure up when compared with peers. Erikson believed that if these industrious children can be successful in their endeavors, they will get a sense of confidence for future challenges. If not, a sense of inferiority can be particularly haunting during middle and late childhood.
Bullying
According to Stopbullying.gov, a federal government website managed by the U.S. Department of Health & Human Services, Bullying is defined as unwanted, aggressive behavior among school-aged children that involves a real or perceived power imbalance. Further, aggressive behavior happens more than once or has the potential to be repeated. There are different types of bullying, including verbal bullying, which is saying or writing mean things, teasing, name calling, taunting, threatening, or making inappropriate sexual comments. Social bullying, also referred to as relational bullying, involves spreading rumors, purposefully excluding someone from a group, or embarrassing someone on purpose. Physical Bullying involves hurting a person’s body or possessions.
A more recent form of bullying is Cyberbullying, which involves electronic technology. Examples of cyberbullying include sending mean text messages or emails, creating fake profiles, and posting embarrassing pictures, videos, or rumors on social networking sites. Children who experience cyberbullying have a harder time getting away from the behavior because it can occur at any time of day and without being in the presence of others. Additional concerns of cyberbullying include that messages and images can be posted anonymously, distributed quickly, and be difficult to trace or delete. Children who are cyberbullied are more likely to experience in-person bullying, be unwilling to attend school, receive poor grades, use alcohol and drugs, skip school, have lower self-esteem, and have more health problems (Stopbullying.gov).
The National Center for Education Statistics and Bureau of Justice statistics indicate that in 2010-2011, 28% of students in grades 6-12 experienced bullying, and 7% experienced cyberbullying. The 2013 Youth Risk Behavior Surveillance System, which monitors six types of health-risk behaviors, indicates that 20% of students in grades 9-12 experienced bullying and 15% experienced cyberbullying (Stopbullying.gov).
Bullying can happen to anyone, but some students are at an increased risk for being bullied including lesbian, gay, bisexual, transgendered (LGBT) youth, those with disabilities, and those who are socially isolated. Additionally, those who are perceived as different, weak, less popular, overweight, or having low self-esteem, have a higher likelihood of being bullied.
Bullies are often thought of as having low self-esteem, and then bully others to feel better about themselves. Although this can occur, many bullies in fact have high levels of self-esteem. They possess considerable popularity and social power and have well-connected peer relationships. They do not lack self-esteem, and instead lack empathy for others. They like to dominate or be in charge of others.
Unfortunately, most children do not let adults know that they are being bullied. Some fear retaliation from the bully, while others are too embarrassed to ask for help. Those who are socially isolated may not know who to ask for help or believe that no one would care or assist them if they did ask for assistance. Consequently, it is important for parents and teachers to know the warning signs that may indicate a child is being bullied. These include unexplainable injuries, lost or destroyed possessions, changes in eating or sleeping patterns, declining school grades, not wanting to go to school, loss of friends, decreased self-esteem and/or self-destructive behaviors.


