3.7: Childbirth and Assessing the Neonate
- Last updated
-
-
Save as PDF
Approaches to Childbirth
Prepared childbirth refers to being not only physically in good condition to help provide a healthy environment for the baby to develop, but also helping expectant parents and caregivers to prepare to accept their new roles and to get information and training that will assist them for delivery and life with the baby as much as possible. The more parents and caregivers can learn about childbirth and the newborn, the better prepared they will be for the adjustment they must make to a new life. Once the knowledge is gained that a child is on the way, people will often begin to conjure up images of what they think the experience will involve. Once the child is born, they must reconcile those images with reality (Galinsky, 1987). Knowing more of what to expect does help them in forming more realistic images thus making the adjustment easier. Let’s explore some of the methods of prepared childbirth.
The Lamaze Method
This method originated in Russia and was brought to the United States in the 1950s by Fernand Lamaze. The emphasis of this method is on teaching the woman to be in control in the process of delivery. It includes learning muscle relaxation, breathing though contractions, having a focal point (usually a picture to look at) during contractions and having a support person who goes through the training process with the mother and serves as a coach during delivery.
Birthing Centers/Birthing Rooms
The trend now is to have birthing rooms that are hospital rooms that look more like a suite in a hotel equipped with a bed that can be converted for delivery. These rooms are also equipped with a bed and monitoring systems for the newborn. However, many hospitals have only one or two of these rooms and availability can be a problem.
The LeBoyer Method
Other birthing options include the use of birthing chairs, which make use of gravity in assisting the woman giving birth and the Leboyer Method of “Gentle Birthing”. This method involves giving birth in a quiet, dimly lit room and allowing the newborn to lie on the mother’s stomach with the umbilical cord intact for several minutes while being given a warm bath.
Home Birth and Nurse-Midwives
Historically in the United States, most babies were born under the care of lay midwives. In the 1920s, middle class women were increasingly using doctors to assist with childbirth but rural women were still being assisted by lay midwives. The nursing profession began educating nurse-midwives to assist these women. Nurse-midwives continued to assist most rural women with delivery until the 1970s and 1980s when their growth is thought to have posed a threat to the medical profession (Weitz, 2007). Since that time, nurse-midwives have found it more difficult to sustain practices with the high costs of malpractice insurance. (Many physicians have changed areas of specialization in response to these costs as well.) Women who are at low risk for birth complications can successfully deliver under the care of nurse-midwives but only 1 percent of births occur at home. Because one out of every 20 births involves a complication, most medical professionals recommend that delivery take place in a hospital. However, some couples choose to have their baby at home. About 1 percent of births occur out of a hospital in the United States. Two-thirds of these are homebirths and more than half of these are assisted by midwives. Midwives are trained and licensed to assist in delivery and are far less expensive than the cost of a hospital delivery. One-third of out-of-hospital births occur in freestanding clinics, birthing centers, or in physicians offices or other locations.
Breech Delivery
Before discussing the stages of labor, we should take a moment to note that some deliveries are "breech". Febrasgo (2015) describes this condition as follows:
Breech delivery, with incidence ranging from 3 to 4% in term gestations, is the second most common delivery presentation. It is a condition in which the baby, at the time of birth, exits the mother’s pelvis buttocks- or feet-first. Based on the relation between the baby’s lower limbs and the bottom, breech presentation can be classified as: complete (the baby’s hips and knees are flexed so that the baby is sitting with feet beside the bottom), and incomplete breech (the baby’s legs are folded flat up against the chest); most breech babies are in the incomplete breech position, with bottom coming first.
Today, the option to deliver a breech baby vaginally is not offered in most cases. The safest way for a breech baby to be born is by C-section (explained below). The danger of breech birth is mostly due to the fact that the largest part of a baby is its head. When the breech baby's pelvis or hips deliver first, the woman's pelvis may not be large enough for the head to be delivered also. This can result in a baby getting stuck in the birth canal, which can cause injury or death. The umbilical cord may also be damaged or blocked. This can reduce the baby's oxygen supply. (Source: MedlinePlus, National Library of Medicine)
As the Breech position is not ideal for delivery, efforts may be made to reorient the baby or a Caesarean section ("C-section") may be planned or required. A C-section is a surgical procedure that involves removing the baby following an incision made in the abdomen. A 2008 article provides some insight into concerns associated with the use of C-sections - in addition to the general issue with making birthing a surgical procedure - and proposed mechanisms for making the C-section more birth-like.
Although much effort has gone into promoting early skin-to-skin contact and parental involvement at vaginal birth, caesarean birth remains entrenched in surgical and resuscitative rituals, which delay parental contact, impair maternal satisfaction and reduce breastfeeding. We describe a ‘natural’ approach that mimics the situation at vaginal birth by allowing (i) the parents to watch the birth of their child as active participants (ii) slow delivery with physiological autoresuscitation and (iii) the baby to be transferred directly onto the mother's chest for early skin-to-skin. Studies are required into methods of reforming caesarean section, the most common operation worldwide.
From: Smith J, Plaat F, Fisk N. The natural caesarean: a woman-centred technique. BJOG 2008;115:1037–1042.
The Process of Delivery
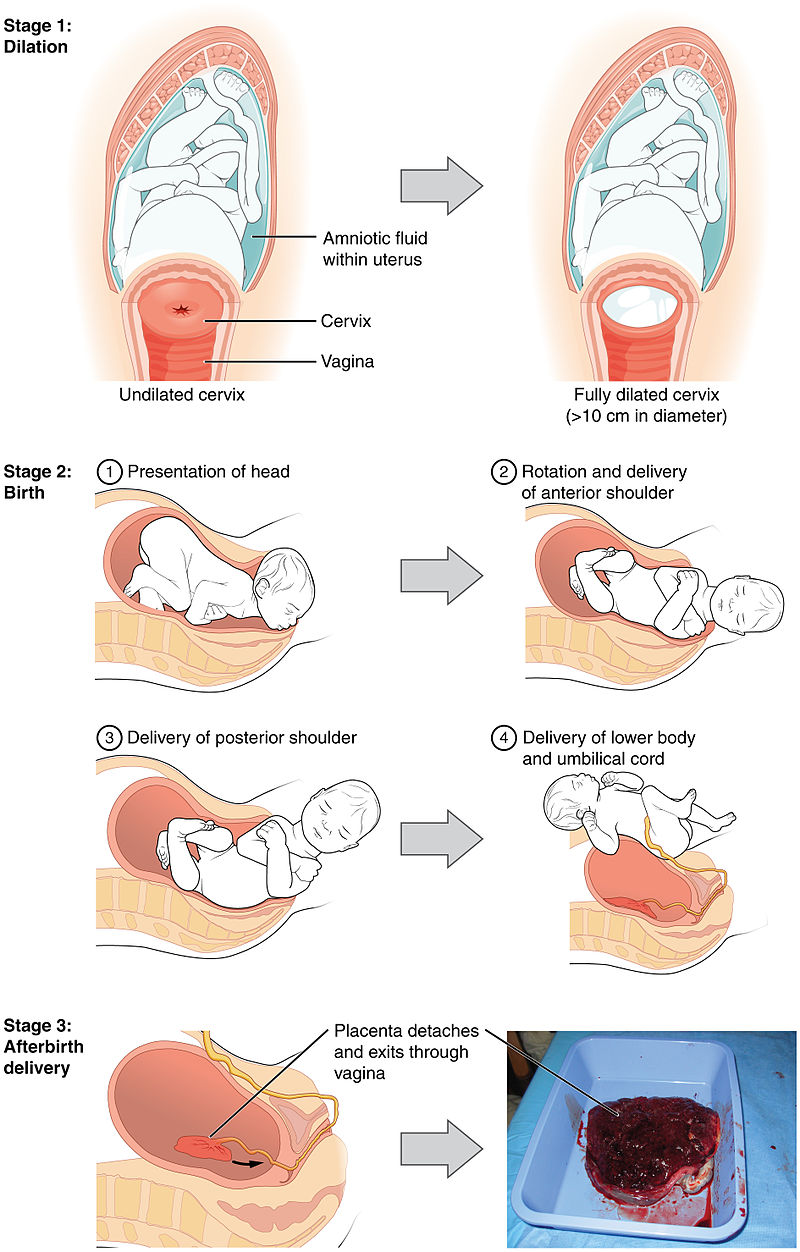
The first stage of labor begins with uterine contractions that may initially last about 30 seconds and be spaced 15 to 20 minutes apart. These increase in duration and frequency to more than a minute in length and about 3 to 4 minutes apart. Typically, doctors advise that they be called when contractions are coming about every 5 minutes. Some women experience false labor or Braxton-Hicks contractions, especially with the first child. These may come and go. They tend to diminish when the mother begins walking around. Real labor pains tend to increase with walking. Labor may also be signaled by a bloody discharge being expelled from the cervix. In one out of 8 pregnancies, the amniotic sac or water in which the fetus is suspended may break before labor begins. In such cases, the physician may induce labor with the use of medication if it does not begin in order to reduce the risk of infection. Normally this sac does not rupture until the later stages of labor.
The first stage of labor is typically the longest. During this stage the cervix or opening to the uterus dilates to 10 centimeters or just under 4 inches. This may take around 12-16 hours for first children or about 6-9 hours for women who have previously given birth. It takes one woman in 9 over 24 hours to dilate completely. Labor may also begin with a discharge of blood or amniotic fluid. If the amniotic sack breaks, labor will be induced if necessary to reduce the risk of infection.
The second stage involves the passage of the baby through the birth canal. This stage takes about 10-40 minutes. Contractions usually come about every 2-3 minutes. The pregnant person pushes and relaxes as directed by the professionals assisting. Normally the head is delivered first. The baby is then rotated so that one shoulder can come through and then the other shoulder. The rest of the baby quickly passes through.
The third stage is relatively painless. During this stage, the placenta or afterbirth is delivered. This typically happenswithin 20 minutes after delivery. If an episiotomy was performed it is stitched up during this stage.
Assessing the Neonate
There are several ways to assess the condition of the newborn. The most widely used tool is the Neonatal Behavioral Assessment Scale (NBAS) developed by T. Berry Brazelton. This tool has been used around the world to help parents get to know their infants and to make comparisons of infants in different cultures (Brazelton & Nugent, 1995). The baby’s motor development, muscle tone, and stress response is assessed. The Apgar is conducted one minute and five minutes after birth. This is a very quick way to assess the newborn’s overall condition. Five measures are assessed: the heart rate, respiration, muscle tone (quickly assessed by a skilled nurse when the baby is handed to them or by touching the baby’s palm), reflex response (the Babinski reflex is tested), and color. A score of 0 to 2 is given on each feature examined. An Apgar of 5 or less is cause for concern. The second Apgar should indicate improvement with a higher score.

