Breast milk is, in most cases, considered the ideal diet for newborns. It has the right amount of calories, fat, and protein to support overall physical and neurological development, it provides a source of iron more easily absorbed in the body than the iron found in dietary supplements, it provides a resistance against many diseases, it is more easily digested by infants than is formula, and it helps babies make a transition to solid foods more easily than if bottle fed.
For nearly all infants, breastfeeding is the best source of nutrition and immunologic protection, and also provides health benefits to mothers (e.g., faster weight loss, reduced risk of breast and ovarian cancers).210 Institutional changes in maternity care practices (e.g., helping mothers initiate breastfeeding within one hour of birth, referring mothers to breastfeeding support groups) increase breastfeeding initiation and duration rates. Support is important to help new mothers establish and continue breastfeeding as they return to work or school. Lactation policies that provide private space and flexible scheduling and that offer lactation management services and support (e.g., breastfeeding peer support programs) can make it easier for a mother to breastfeed.
Figure \(\PageIndex{1}\): In order to increase breastfeeding, it is important that mothers feel comfortable doing so in public places. (Unsplash license; Dave Clubb via Unsplash)
In the United States, the American Academy of Pediatrics (AAP) currently recommends:1
Infants should be fed breast milk exclusively for the first 6 months after birth. Exclusive breastfeeding means that the infant does not receive any additional foods (except vitamin D) or fluids unless medically recommended.
After the first 6 months and until the infant is 1 year old, the AAP recommends that the mother continue breastfeeding while gradually introducing solid foods into the infant's diet.
After 1 year, breastfeeding can be continued if mutually desired by the mother and her infant.
The World Health Organization currently promotes as a global public health recommendation that:2
Infants be exclusively breastfed for the first 6 months after birth to achieve optimal growth, development, and health.
After the first 6 months, to meet their evolving nutritional requirements, infants should receive nutritionally adequate and safe complementary foods while breastfeeding continues for up to 2 years of age or beyond.
However, most mothers who breastfeed in the United States stop breast feeding at about 6-8 weeks, often in order to return to work outside the home. Mothers can certainly continue to provide breast milk to their babies by expressing and freezing the milk to be bottle fed at a later time or by being available to their infants at feeding time, but some mothers find that after the initial encouragement they receive in the hospital to breast feed, the outside world is less supportive of such efforts. Some workplaces support breastfeeding mothers by providing flexible schedules and welcoming infants, but sadly, most do not. And public support of breastfeeding is still widely lacking, although social awareness of this issue seems to be changing perceptions in positive ways. Women in Canada are more likely to breastfeed than are those in the United States and the Canadian health recommendation is for breastfeeding to continue until 2 years of age. Facilities in public places in Canada such as malls, ferries, and workplaces provide more support and comfort for the breastfeeding mother and child than found in the United States.
One early argument given to promote the practice of breastfeeding was that it promoted bonding and healthy emotional development for infants. However, this does not seem to be the case. Breastfed and bottle-fed infants adjust equally well emotionally (Ferguson and Woodward, 1999). This is good news for mothers who may be unable to breastfeed for a variety of reasons and for fathers and other caregivers who might feel left out as a result.
In addition to the nutritional benefits of breastfeeding, breast milk is free! Anyone who has priced formula recently can appreciate this added incentive to breastfeeding. Prices for a month’s worth of formula can easily range from $130-200. Breastfeeding also stimulates contractions in the uterus to help it regain its normal size. And women who breastfeed are more likely to space their pregnancies further apart.
A Historic Look at Breastfeeding
The use of wet nurses, or lactating women hired to nurse others’ infants, during the middle ages eventually declined and mothers increasingly breastfed their own infants in the late 1800s. In the early part of the 20th century, breastfeeding began to go through another decline and by the 1950s, it was practiced less frequently by middle class, more affluent mothers as formula began to be viewed as superior to breast milk (education in this area has since changed). In the late 1960s and 1970s, greater emphasis began to be placed on natural childbirth and breastfeeding and the benefits of breastfeeding were more widely publicized. Gradually rates of breastfeeding began to climb, particularly among middle-class educated mothers who received the strongest messages to breastfeed. Today, women receive consultation from lactation specialists before being discharged from the hospital to ensure that they are informed of the benefits of breastfeeding and given support and encouragement to get their infants to get used to taking the breast. This does not always happen immediately and first-time mothers, especially, can become upset or discouraged. In this case, lactation specialists and nursing staff can encourage the mother to keep trying until the baby and mother are comfortable with the feeding.
Global Considerations and Malnutrition
In the 1960s, formula companies led campaigns in developing countries to encourage mothers to feed their babies on infant formula. Many mothers felt that formula would be superior to breast milk and began using formula. The use of formula can certainly be healthy under conditions in which there is adequate, clean water with which to mix the formula and adequate means to sanitize bottles and nipples. However, in many of these countries such conditions were not available and babies often were given diluted, contaminated formula which made them become sick with diarrhea and become dehydrated. Rates of breastfeeding declined in Peru from 90 percent to 10 percent in just 8 years' time (Berger, 2001). These conditions continue today and now many hospitals prohibit the distribution of formula samples to new mothers in efforts to get them to rely on breastfeeding. Many of these mothers may not understand the benefits of breastfeeding and have to be encouraged and supported in order to promote this practice. Breastfeeding could save the lives of millions of infants each year, according to the World Health Organization, yet fewer than 40 percent of infants are breastfed exclusively for the first 6 months of life. Find out more at theWHO’s 10 facts on breastfeeding. Most women can breastfeed (if the case is that they are physically able) unless they are receiving chemotherapy or radiation therapy, have HIV, are dependent on illicit drugs, or have active, untreated tuberculosis.
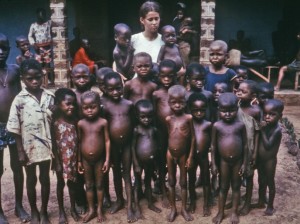
Children in developing countries and countries experiencing the harsh conditions of war are at risk for two major types of malnutrition. Infantile marasmus refers to starvation due to a lack of calories and protein. Children who do not receive adequate nutrition lose fat and muscle until their bodies can no longer function. Babies who are breastfed are much less at risk of malnutrition than those who are bottle-fed. After weaning, children who have diets deficient in protein may experience kwashiorkor or the “disease of the displaced child” often occurring after another child has been born and taken over breastfeeding. This results in a loss of appetite and swelling of the abdomen as the body begins to break down the vital organs as a source of protein.
Figure \(\PageIndex{2}\): Kwashiorkor (Photo Courtesy Centers for Disease Control and Prevention)
Cognitive Development in Infancy - Piaget and Sensorimotor Intelligence
Remember our discussion of sensorimotor development during the first two years of life? Piaget describes intelligence in infancy as sensorimotor or based on direct, physical contact. Infants taste, feel, pound, push, hear, and move in order to experience the world. Let’s explore the transition infants make from responding to the external world reflexively as newborns to solving problems using mental strategies as two-year-olds.
As discussed earlier, Piaget believed his stages were biologically defined and that children pass through them in a very specific way. He also proposed that they construct their knowledge of the world through two processes, assimilation and accommodation. Assimilation refers to incorporating new knowledge into your existing knowledge without changing it. We can think of this knowledge in terms of schemes - mental or physical ways of interacting with the world. In this 1st stage, we see assimilation when an infant mouths a block or a ball in the same way it mouths a pacifier. The knowledge is the infants approach to exploring - and the infant does the same thing no matter what the object. When an infant encounters something that causes that approach to change - such as discovering that it hurts to mouth some things, then we have accommodation. Accommodation happens when the knowledge changes due to a new experience.
Stage One: Reflexive Action: (Birth through 1st month)
This active learning begins with automatic movements or reflexes. A ball comes into contact with an infant’s cheek and is automatically sucked on and licked. But this is also what happens with a sour lemon, much to the infant’s surprise!
Stage Two: First Adaptations to the Environment (1st through 4th month)
Fortunately, within a few days or weeks, the infant begins to discriminate between objects and adjust responses accordingly as reflexes are replaced with voluntary movements. An infant may accidentally engage in a behavior and find it interesting such as making a vocalization. This interest motivates trying to do it again and helps the infant learn a new behavior that originally occurred by chance. At first, most actions have to do with the body, but in months to come, will be directed more toward objects.
Stage Three: Repetition (4th through 8th months)
During the next few months, the infant becomes more and more actively engaged in the outside world and takes delight in being able to make things happen. Repeated motion brings particular interest as the infant is able to bang two lids together from the cupboard when seated on the kitchen floor.
Stage Four: New Adaptations and Goal-Directed Behavior (8th through 12th months)
Now the infant can engage in behaviors that others perform and anticipate upcoming events. Perhaps because of continued maturation of the prefrontal cortex, the infant becomes capable of having a thought and carrying out a planned, goal-directed activity such as seeking a toy that has rolled under the couch. The object continues to exist in the infant’s mind even when out of sight and the infant now is capable of making attempts to retrieve it. Here is an example of a lack of object permanence.
Was Piaget Correct?
Infants seem to be able to recognize that objects have permanence at much younger ages (even as young as 3.5 months of age). Dr. Rene Baillargeon explains in the following clip:
Video \(\PageIndex{1}\): Object Concept VOE Ramp Study Baillargeon
Stage Five: Active Experimentation of Little Scientists (12th through 18th months)
Infants from one year to 18 months of age more actively engage in experimentation to learn about the physical world. Gravity is learned by pouring water from a cup or pushing bowls from high chairs. The caregiver tries to help the child by picking it up again and placing it on the tray. And what happens? Another experiment! The child pushes it off the tray again causing it to fall and the caregiver to pick it up again! A closer examination of this stage causes us to really appreciate how much learning is going on at this time and how many things we come to take for granted must actually be learned. This is a wonderful and messy time of experimentation and most learning occurs by trial and error.
Stage Six: Mental Representations (18th month to 2 years of age)
The child is now able to solve problems using mental strategies, to remember something heard days before and repeat it, to engage in pretend play, and to find objects that have been moved even when out of sight. Take for instance, the child who is upstairs in a room with the door closed, supposedly taking a nap. The doorknob has a safety device on it that makes it impossible for the child to turn the knob. After trying several times in vain to push the door or turn the doorknob, the child carries out a mental strategy to get the door opened and knocks on the door! Obviously, this is a technique learned from the past experience of hearing a knock on the door and observing someone opening the door. The child is now better equipped with mental strategies for problem-solving. This initial movement from the “hands-on” approach to knowing about the world to the more mental world of stage six marked the transition to preoperational intelligence that we will discuss in the next lesson. Part of this stage involves learning to use language.
Conclusions About Piaget
Piaget is noteworthy as he proposed a comprehensive view of how thinking (cognition) develops. And as the pioneer in this area of study, his ideas have been tested extensively. While it appears that he underestimated infants, we'll discover that he ultimately overestimates teens. While aspects of his theory may need modification, it does provide us with a way of thinking about infant thinking. In infancy, knowing is sensing and doing - and object permanence is lacking. Mental representation, actual thinking, begins as we move to Piaget's next stage, preoperational.

 Figure \(\PageIndex{1}\): In order to increase breastfeeding, it is important that mothers feel comfortable doing so in public places. (Unsplash license; Dave Clubb via Unsplash)
Figure \(\PageIndex{1}\): In order to increase breastfeeding, it is important that mothers feel comfortable doing so in public places. (Unsplash license; Dave Clubb via Unsplash)