
16.2: Health Consequences of the Transition to Agriculture and Animal Domestication
- Page ID
- 177794
THE TRANSITION TO AGRICULTURE AND ANIMAL DOMESTICATION
Living in groups settled permanently in one place.
EPIDEMIOLOGICAL TRANSITIONS
Changes in diet and physical-activity patterns associated with agriculture, in conjunction with increased population densities and exposure to zoonoses, resulted in what is known as an epidemiological transition, a shift in the causes of morbidity and mortality among humankind (Omran 1971). The first epidemiological transition from foraging to food production resulted in increases in dental caries, nutritional deficiencies, infectious disease, and skeletal conditions like osteoarthritis, as well as decreases in growth and height (Larsen 2014). A second epidemiological transition occurred following the Industrial Revolution in Western Europe and the United States when socioeconomic, political, and cultural conditions contributed to improved standards of living, hygiene, and nutrition that minimized the effects of infectious disease, after which people began to experience the Noncommunicable Diseases (NCDs) that are the focus of the remainder of this chapter (Omran 2005). With the addition of immunizations and other public health initiatives, modified forms of this transition remain ongoing in many low- and middle-income countries (Zuckerman et al. 2014), with several now facing a “double burden” of disease, with poor, often rural, populations falling prey to infectious diseases, while more affluent citizens are victims of chronic illnesses. A third epidemiological transition is now underway as infectious diseases, some of them novel, others re-emergent, and others even multi-drug resistant, have once again become major health concerns (Harper and Armelagos 2010; Zuckerman et al. 2014). These include Ebola, HIV/AIDS, tuberculosis, malaria, dengue, Lyme disease, and West Nile virus, all zoonoses that initially spread to humans through contact with animals. These diseases are increasing their geographic ranges due to climate change, economic development, and deforestation (Baer and Singer 2009).
Also known as chronic diseases, NCDs tend to be of long duration and are the result of a combination of genetic, physiological, environmental, and behavior factors. The main types of NCDs are cardiovascular diseases
Refers to parts of the world in which there is a prevalence of chronic disease (e.g.,. cancer, heart disease) while, at the same time, there are also high rates of infectious disease due to poverty, malnutrition, poor sanitation, and lack of access to health care, often accompanied by high rates of maternal and child mortality.
Patterns of morbidity and mortality continue to shift across the globe. As with the first epidemiological transition resulting from the adoption of large-scale agriculture, such shifts can be the direct, if unintended, result of human interactions with the environment. For example, there has been a well-documented rise in chronic inflammatory diseases (CIDs) in recent decades in developed countries (Versini et al. 2015). This includes increased rates of allergic conditions like asthma, as well as autoimmune diseases like rheumatoid arthritis, multiple sclerosis, Crohn’s disease, and inflammatory bowel disease. This has coincided with the decrease in infectious disease associated with the second epidemiological transition, and the two are related. The “hygiene hypothesis” postulates the rise in CIDs is a result of limited exposure to nonlethal environmental pathogens in utero and early childhood (Zuckerman and Armelagos 2014). Modern human societies have become so sanitized that we are no longer exposed to microorganisms that stimulate the development of a healthy immune system (Versini et al. 2015). “In effect, the lifestyle changes—sanitary improvements, pasteurization, use of antibiotics, and improved hygiene—that contributed to the second transition may have produced a substantial trade-off in health and quality of life, with developed nations exchanging a high burden of infectious disease for a higher burden of CIDs” (Zuckerman et al. 2014).
Similarly, the re-emergence of infectious disease, the third epidemiological transition, reflects the continuing relationship between humans, animals, and pathogens. Over 60% of Emerging Infectious Diseases (EIDs) between 1940 and 2004 have been of zoonotic origin, with over 70% stemming from human contact with wildlife (Jones et al. 2008). The global bushmeat trade currently devastating Africa’s wildlife is a continuing source of Ebola infection (Asher 2017), as well as the original source of HIV and viruses related to leukemia and lymphoma among humans (Zuckerman et al. 2014). Further, new strains of avian (bird) flu, some with mortality rates as high as 60% among human victims (WHO n.d.), are transmitted to humans through poultry production and contact with wild birds; these pose a looming global threat of epidemic disease (Davis 2005). Lastly, the use of antibiotics in commercial meat production is directly related to the rise of drug-resistant strains of previously controlled infectious diseases. An estimated 80% of antibiotics in the U.S. are used to promote growth and prevent infection in livestock, and drug-resistant bacteria from these animals are transmitted to humans through meat consumption (Ventola 2015).
Infections that have recently appeared within a population or those whose incidence or geographic range is rapidly increasing or threatens to increase in the near future. Examples include Ebola, Zika, SARS, and avian (bird) flu.
These examples illustrate continuing interaction between humans, our evolved biology, and the physical and cultural environments in which we live. The remainder of this chapter will focus on selected noncommunicable diseases and the social, cultural, and environmental factors that contribute to their prevalence in modern, industrialized economies. We begin with the health condition that affects all of the others—obesity.
The proportion of individuals in a population who have a particular disease or condition at a given point in time.
A medical condition in which excess body fat has accumulated to the point that it has adverse effects on health. The most widely used measure for identifying obesity is the Body Mass Index (BMI), a person’s weight in kilograms divided by the square of their height in meters. A measure of 30 kg/m2 is considered obese and 25—29 kg/m2 overweight. Distribution of body fat also matters. Fat in the abdominal region has a stronger association with Type 2 diabetes and cardiovascular disease, meaning waist to hip ratio and waist circumference are also important indicators of obesity-related health risk.
OBESITY
According to the World Health Organization (2017b), 1.9 billion of the world’s people are overweight and 650 million of these are obese. In the United States, 70% of Americans are overweight, and 40% of these meet the criteria for obesity. For the first time in human history, most of the world’s population lives in countries where overweight and obesity kill more people than hunger does (see Figure \(\PageIndex{1}\)). Improvements in public health and food production have allowed a greater number of people to live past childhood and to have enough food to eat. This does not include everyone. Many people still struggle with poverty, hunger, and disease, even in the wealthiest of nations, including the United States. On a global scale, however, many people not only have enough food to survive but also to gain weight—and, notably, enough extra weight to cause significant health problems. Several aspects of life in modern, industrialized societies contribute to the obesity crisis.
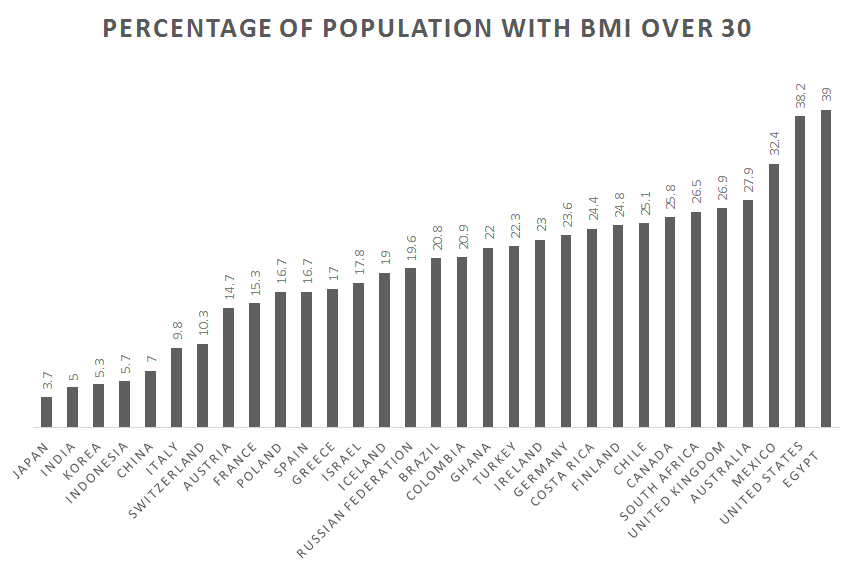 Figure \(\PageIndex{1}\): Obesity rates by country, 2017.
Figure \(\PageIndex{1}\): Obesity rates by country, 2017.Causes of Obesity
Although studies show differences in daily energy expenditure between modern foraging and farming populations in comparison with industrialized peoples, the major contributor to obesity in Western populations is energy intake (Pontzer et al. 2012). Many people not only eat too much but too much of the wrong things. Biological anthropologist Leslie Lieberman (2006) argues that contemporary humans continue to rely on cues from foraging strategies in our evolutionary past that are now counterproductive in the obesogenic environments in which we now live.
Promoting excessive weight gain. For example, an environment in which tasty, cheap food filled with excess calories is abundant.
Examine your own eating habits in the context of how humans once hunted and gathered. We relied on visual cues to find food, often traveling long distances to obtain it, then transporting it back to our home base. There we may have had to process it, by hand, to render it edible. Think of how much less energy it takes to find food now. If we have the financial resources, we can acquire big energy payoffs by simply sitting at home and using an app on our mobile phone to place an order for delivery. And, voila! High-calorie (if not highly nutritious) food arrives at our door within minutes. Should we venture out for food, search time is reduced by signage and advertising directing us toward high-density “patches” where food is available 24 hours a day. These include vending machines, gas stations, and fast-food outlets. Travel time is minimal and little human energy is used in the process (Lieberman 2006).
Foods are also prepackaged and prepared in ways that allow us to eat large quantities quickly. Think French fries or chicken nuggets, which we can easily eat with our hands while doing other things, like driving or watching television, rendering eating mindless and allowing us to take in food faster than our endocrine systems can let us know we are getting full. Modern “patches” offer low-fiber, calorie-dense resources, which allows us to eat larger quantities, a problem already encouraged by our larger portion sizes (Lieberman 2006). Processed foods are also engineered to appeal to hominin preferences for sweet tastes and fatty, creamy textures (Moss 2013). Remember from earlier chapters that natural selection favored depth perception, color vision, grasping hands, and coordinated eye-hand movements as general primate traits. Advertising and packaging now use our color vision against us, attracting us to products with little nutritional value and playing to our evolutionary predisposition toward variety. Remember those 50 different nutrients we require? That variety is now presented to us in the form of 55 different flavors of Oreo cookies (Cerón 2017), which we take out of the package and dip in milk using our hand-eye coordination and depth perception.
Those organs in the body whose primary function is the production of hormones.
Even if we are ostensibly eating the same things our ancestors did, these foods may not be all that much alike. Take potatoes, for example. One medium-sized, plain, baked potato is a healthy food, especially if we eat the skin too. It contains 110 calories, 0 grams of fat, 26 grams of carbohydrates, and 3 grams of protein, plus 30% of the U.S. Recommended Daily Allowance (RDA) of vitamin C, 10% of vitamin B6, 15% of potassium, and no sodium (http://www.potatogoodness.com). In contrast, a medium order of McDonald’s fries, which takes the potato and adds salt and fat, contains 340 calories, 16 grams of fat, 44 grams of carbohydrates, 4 grams of protein, and 230 mg of sodium (http://www.mcdonalds.com). Potato chips take food processing to a whole new level, removing even more nutrition and adding a host of additional ingredients, including oils, preservatives, and artificial flavorings and colors (Moss 2013). Let us use Ruffles Loaded Bacon and Cheddar Potato Skins Potato Chips, one of the top new flavors of 2018, as an example (St. Pierre 2018). The number of ingredients increases from one to 11 to 35 as we move from the potato to the potato chip, moving further from nature with each step (Table \(\PageIndex{1}\)). It should be noted that the nutritional information for the potato chips is based on a serving size of 11 chips, an amount likely smaller than many people eat. Our bodies also do not react to fries and chips the same way they do to potatoes. Added fat and calories translate into overweight and obesity. Sodium contributes to hypertension. And, artificial flavorings and colorings, including the Yellow 5 and Yellow 6 in the chips, have been linked to cancer, as well as allergies and hyperactivity in children (CSPI 2010). Many sweet, fatty, salty foods like fries and chips are cheap and easily available, which is why many people choose to eat them (Moss 2013). The price of a medium-sized order of McDonald’s fries as of this writing is US$1.79, and the potato chips are $2.98 for an 8.5-ounce bag. A single potato prewrapped for microwaving is available in many supermarkets for US$1.99 but requires travel to a market and access to a microwave and eating utensils, making it less convenient.
|
Baked Potato [baked, skin on, plain] |
French Fries [medium order] |
Potato Chips [1 oz. serving of 11 chips] |
|
| Calories | 110 | 340 | 160 |
| Calories from fat | 0 | 144 | 90 |
| Fat | 0 g | 16 g | 10 g |
| Carbohydrates | 26 g | 44 g | 15 g |
| Protein | 3 g | 4 g | 2 g |
| Sodium | 0 g | 230 mg | 170 mg |
| Dietary fiber | 2 g | 4 g | 1 g |
| Sugars | 1 g | 0 g | 1 g |
| Cholesterol | 0 g | 0 g | 0 g |
| Ingredients | Potato | Potatoes, Vegetable Oil (Canola Oil, Soybean Oil, Hydrogenated Soybean Oil, Natural Beef Flavor [Wheat and Milk Derivatives]*, Citric Acid [Preservative]), Dextrose, Sodium Acid Pyrophosphate (Maintain Color), Salt. | Potatoes, Vegetable Oil (Sunflower, Corn, and/or Canola oil), Bacon & Cheddar Loaded Potato Skins Seasoning (Maltodextrin [Made from Corn], Salt, Cheddar Cheese [Milk, Cheese Cultures, Salt, Enzymes], Sour Cream [Cultured Cream, Skim Milk], Whey, Dried Onion, Monosodium Glutamate, Natural Flavor [including Natural Smoke Flavor], Skim Milk, Corn Oil, Canola Oil, Sugar, Buttermilk, Yeast Extract, Romano Cheese [Part-Skim Cow’s Milk, Cheese Cultures, Salt Enzymes], Whey Protein Concentrate, Dextrose, Spice, Citric Acid, Lactic Acid, Artificial Color [Yellow 5 Lake, Yellow 5, Yellow 6, Yellow 6 Lake], Butter [Cream, Salt], Sodium Caseinate, Garlic Powder, Blue Cheese [Milk, Cheese Cultures, Salt, Enzymes], and Bacon Fat. |


Not only have we transformed the food supply and our eating in ways that are detrimental to our health, but these changes have been accompanied by reductions in physical activity. Sedentarism is built into contemporary lifestyles. Think of how much time you spent sitting down today. Some of it may have been in class or at work, some may have been driving a car or perhaps binge-watching your favorite show, playing a video game, or checking in on social media. An inactive lifestyle is almost dictated by the digital age (Lucock et al. 2014). Levels of physical activity in many countries are now so low that large portions of the population are completely sedentary, including 28% of Americans (Physical Activity Council 2018). For a species whose biology evolved in an environment where walking, lifting, and carrying were part of daily life, this is unhealthy and often leads to weight gain.
Obesity varies by gender, age, geography, and, to some degree, ethnicity (Brown 1991). In general, women tend to gain weight easier than men, but fat distribution is different between them. Women tend to put on weight in the thighs and hips, while men gain weight around their abdomen. The latter is a much greater health risk (Akil and Ahmad 2011). Weight gain also varies across the lifespan, with infants and toddlers tending toward chubbiness then becoming slimmer until adolescence and the onset of puberty (Lucock et al. 2014). This pattern is the result of selective pressure to maintain energy for brain development in early life, then again later on for reproduction. There is also the “thrifty gene” hypothesis: the idea that natural selection favored genotypes that clung to every calorie available to protect against the constant threat of food shortages throughout our evolutionary history, and that this was a species-wide adaptation (Neel 1962).

Figure \{\PageIndex{2}\} Participants of a walk against diabetes and for general fitness around Nauru airport.
More recent genetic research indicates there are multiple genetic variants that influence weight gain, and they are not spread evenly across or within human populations. Tuomo Rankinen and colleagues (2006) identified 127 genes associated with obesity, of which 22 were supported by research indicating that they contributed to positive energy balance and weight gain. Claude Bouchard (2007) went further, identifying five categories of obesity-promoting genotypes. These include genotypes that promote sedentarism, result in low metabolism, and lead to poor regulation of appetite and satiety and a propensity to overeat. An example of the impact such genotypes can have in an environment of plenty is found among the population of the Micronesian island of Nauru. Historically, the island was geographically isolated and the food supply was unpredictable. These conditions favored genotypes that promoted the ability to rapidly build up and store fat in times of food availability. In Nauruans, there are two genetic variations favoring weight gain and insulin resistance, and both are associated with obesity and Type 2 diabetes. One variant is also associated with higher diastolic blood pressure. One of these variants is also found in Pima Indians in the United States, where it is associated with a high Body Mass Index (BMI) and Type 2 diabetes, although it is not associated with the same outcomes in Japanese and British subjects (de Silva et al. 1999). The other variant was also analyzed in Finnish and South Indian populations, neither of whom experienced the same outcome as Nauruans. This suggests these alleles may act as modifying genes for Type 2 diabetes in some population groups (Baker et al. 1994). Unfortunately, Nauruans are one of those groups. Eventually, they became wealthy through phosphate mining on the island, gaining access to a calorie-rich Western diet of imported foods and developing a sedentary lifestyle. This resulted in rates of Type 2 diabetes as high as 30–40% of Nauruans over the age of 15, which became the leading cause of death (Lucock et al. 2014), something Nauruans are taking seriously (See Figure \{\PageIndex{2}\}).
A person’s weight in kilograms divided by the square of their height in meters. The most widely used measure for identifying obesity. The formula using kilograms and meters (or centimeters) is: weight (kg) / [height (m)]2 . The formula using pounds and inches is: 703 x weight (lbs) / [height (in)]2 .
Factors other than biology influence which populations carry and express a genetic predisposition toward obesity and which populations carry but do not express it. The Pima Indians, for example, were seriously impacted by U.S. government policies that affected water rights, forcing the population away from subsistence farming to dependence on government commodities and convenience food. This resulted in a significant loss of physical activity and sedentarism, as well as malnutrition and obesity. Those living on the reservation continue to experience hardship due to high rates of unemployment and poverty, as well as depression, sometimes made worse by alcoholism. In the absence of these pressures, the Pima were diabetes free for centuries prior, even though they relied on agriculture for subsistence, suggesting genetics alone is not responsible for high rates of obesity and diabetes in current populations (Smith-Morris 2004).
Obesity also has an epigenetic component. You learned about epigenetics in Chapter 3. With regard to obesity, epigenetics is counterintuitive in that mothers who do not take in enough calories during pregnancy often give birth to babies who grow up to be fat. What takes place is that the fetus receives signals from the mother through the placenta and intrauterine environment about environmental conditions during pregnancy, in this case food insecurity. These signals encourage the turning on and off of genes related to metabolism, for example. This alters the phenotype of the fetus so that if the child is born into an environment where food is readily available, it will put on weight rapidly whenever possible, falling prey to obesity and related diseases later in life. What is worse is that if the child is a girl, her own eggs are formed in utero with the same genetic changes coded in, meaning she will pass along this same genetic predisposition to gain weight to her children. Hence, a biological propensity toward obesity can continue across generations (Worthman and Kuzara 2005). This same mechanism operates in populations born into poverty that are now growing into plenty. Epigenetic changes to genes that promote weight gain are argued to be partly responsible for the rapid rise in obesity and diabetes in recent years in developing countries gaining access to Western diets (Stearns et al. 2008).
Obesity and overweight put a tremendous strain on several biological systems of the body, including the circulatory, endocrine, and skeletal systems, contributing to hypertension, heart disease, stroke, diabetes, and osteoarthritis (Figure \{PageIndex{3}\}). Obesity also elevates the risk of cancers of the breast, endometrium, kidney, colon, esophagus, stomach, pancreas, and gallbladder (National Institutes of Health 2017; Vucenik and Stains 2012). Diabetes, one of the fastest growing health conditions around the globe (WHO 2016) and one tightly connected to obesity and overweight, is the focus of the following Special Topics feature.
A stroke occurs when a blood vessel leading to the brain is blocked or bursts, preventing that part of the brain from receiving blood and oxygen, leading to the death of cells in that part of the brain.
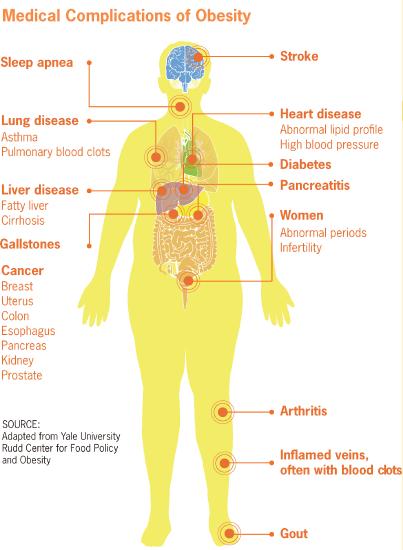 Figure \{PageIndex{3}\}: Medical Complications of Obesity.
Figure \{PageIndex{3}\}: Medical Complications of Obesity.Diabetes Mellitus is an endocrine disorder characterized by excessively high blood glucose levels (Martini et al. 2013). According to a report released by the World Health Organization, the number of people living with diabetes is growing in all regions of the world. Rates of diabetes have nearly doubled in the past three decades, largely due to increases in obesity and sugary diets (WHO 2016). One in 11 people around the world, 435 million people, now have diabetes, including over 30 million Americans. In the United States, the disease is rising fastest among millennials (those ages 20-40) (BCBSA 2017), and one in every two adults with diabetes is undiagnosed (IDF 2018). Obesity and diabetes are linked: that is, obesity causes a diet-related disease (diabetes) because of humans’ evolved metabolic homeostasis mechanism, which is mismatched to contemporary energy environments (Lucock et al. 2014).
An endocrine disorder in which high glucose (blood sugar) levels occur over a prolonged period of time. Blood glucose is your body’s main source of energy and comes from the food you eat. Insulin, a hormone made by the pancreas, helps glucose from food get into your cells to be used for energy. Sometimes your body does not make enough—or any—insulin (Type 1 diabetes) or does not take up insulin well (Type 2 diabetes). Glucose then stays in your blood and does not reach your cells.
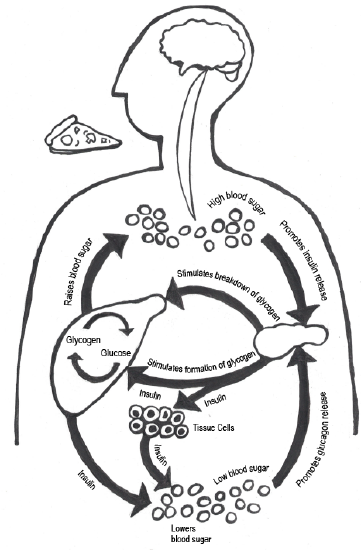 Figure \{\PageIndex{4}\}: Glucose metabolism is the body’s evolved mechanism by which we turn food into energy for bodily functions. Carbohydrates are eaten and broken down into simple sugars (e.g., glucose). Glucose enters the bloodstream from the intestines, and the increase in glucose stimulates the pancreas to release insulin into the bloodstream. Insulin deposits glucose in the muscles and fat cells, where it is stored and used for energy.
Figure \{\PageIndex{4}\}: Glucose metabolism is the body’s evolved mechanism by which we turn food into energy for bodily functions. Carbohydrates are eaten and broken down into simple sugars (e.g., glucose). Glucose enters the bloodstream from the intestines, and the increase in glucose stimulates the pancreas to release insulin into the bloodstream. Insulin deposits glucose in the muscles and fat cells, where it is stored and used for energy.To function properly, cells need a steady fuel supply. Blood sugar is the primary fuel for most cells in the body, and the body produces the hormone insulin to help move energy into cells that need it. Insulin functions like a key, turning on insulin receptors located on the surface of the cell. The receptor then activates glucose transporters (GLUTs) that do the work of hauling glucose (blood sugar) out of your bloodstream and into your cells (McKee and McKee 2015; see Figure \{PageIndex{4}\}). Foods that most readily supply glucose to your bloodstream are carbohydrates, especially starchy foods like potatoes or sweet, sugary foods like candy and soda. The body can also convert other types of foods, including protein-rich foods (e.g., lean meats) and fatty foods (e.g., vegetable oils and butter), into blood sugar in the liver via gluconeogenesis. Insulin’s main job is to tell your cells when to take up glucose. The cell also has to listen to the signal and mobilize the glucose transporters. This not only allows your cells to get the energy they need, but it also keeps blood sugar from building up to dangerously high levels when you are at rest. Muscles can use glucose without insulin when you are exercising; it does not matter if you are insulin resistant or if you do not make enough insulin. When you exercise, your muscles get the glucose they need, and, in turn, your blood glucose level goes down. If you are insulin resistant, resistance goes down when you exercise and your cells use glucose more effectively (Leontis n.d.).
The body’s evolved mechanism by which we turn food into energy for bodily functions.
A hormone produced in the pancreas that regulates the amount of glucose in the blood. Lack of insulin or the inability to absorb insulin causes diabetes.
This system is efficient, but there are limits. Keep in mind that, like the rest of our biology, it evolved during several million years when sugar was hard to come by and carbohydrates took the form of fresh foods with a low glycemic index (GI). Our ancestors were also active throughout the day, taking pressure off of the endocrine system. Now, sedentary lifestyles and processed-food diets cause many of us to take in more calories—and especially more carbohydrates—than our bodies can handle. The fact is, there is only so much blood sugar your cells can absorb. As soaring rates of diabetes show, many modern populations are taxing those limits. After years of being asked by insulin to take in more glucose than they can use, cells eventually stop responding (McKee and McKee 2015). This is called Type 2 diabetes or insulin resistance, which accounts for 90–95% of diabetes cases in the United States. People with Type 1 diabetes do not produce insulin (O’Keefe Osborn 2017; see Figure 16.8).
A system that ranks foods on a scale from 1 to 100 based on their effect on blood-sugar levels. Carbohydrates with a low GI value (55 or less) are more slowly digested and metabolised causing a lower, slower rise in blood glucose and insulin levels.
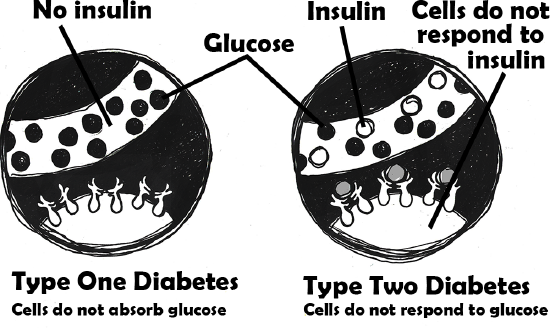 Figure \{\PageIndex{5}\}: Type 1 and Type 2 Diabetes.
Figure \{\PageIndex{5}\}: Type 1 and Type 2 Diabetes.Type 2 diabetes is a progressive metabolic condition that occurs over time when our evolved biological mechanism that turns food into energy is derailed by the obesogenic environments in which we live. This is compounded by a sedentary lifestyle. Think about how living in a college environment contributes to the development of diabetes. How much time do you spend sitting each day? How many sugary—and often cheap—carbohydrates are within easy reach? Making simple changes now can head off health complications later. Carrying an apple or orange in your backpack instead of a candy bar and walking or biking instead of driving can make a big difference.
REFERENCES
Akil, Luma, and H. Anwar Ahmad. 2011. “Relationships between Obesity and Cardiovascular Diseases in Four Southern States and Colorado.” Journal of Health Care for the Poor and Underserved 22 (Suppl. 4): 61–72.
Armelagos, George J., Peter J. Brown, and Bethany Turner. 2005. “Evolutionary, Historical and Political Economic Perspectives on Health and Disease.” Social Science and Medicine 61 (4): 755–765.
Asher, Claire. 2017. “Illegal Bushmeat Trade Threatens Human Health and Great Apes.” Mongabay, April 6. https://news.mongabay.com/2017/04/il...nd-great-apes/.
Baer, Hans, and Merrill Singer. 2009. Global Warming and the Political Ecology of Health: Emerging Crises and Systemic Solutions. Walnut Creek, CA: Left Coast Press.
Baker, W.A., G.A. Hitman, K. Hawrami, M.I. McCarthy et al. 1994. “Apolipoprotein D Gene Polymorphism: A New Genetic Marker for Type 2 Diabetic Subjects in Nauru and South India.” Diabetic Medicine 11 (10): 947–952.
Blue Cross Blue Shield Association (BCBSA). 2017. “Diabetes and the Commercially Insured U.S. Population.” The Health of America Report, August 1. https://www.bcbs.com/the-health-of-a...-us-population.
Bouchard, Claude. 2007. “The Biological Predisposition to Obesity: Beyond the Thrifty Genotype Scenario.” International Journal of Obesity 31: 1337–1339.
Brown, Peter J. 1991. “Culture and the Evolution of Obesity.” Human Nature 2 (1): 31–57.
Center for Science in the Public Interest (CSPI). 2010. Food Dyes: A Rainbow of Risk. Washington, DC: Center for Science in the Public Interest.
Cerón, Ella. 2017. “Here’s Every Oreo Flavor Ever Created.” TeenVogue.com, June 19. https://www.teenvogue.com/story/ever...-flavor-ranked.
Cooling, Laura. 2015. “Blood Groups in Infection and Host Susceptibility.” Clinical Microbiology Reviews 28 (3): 801–870.
Davis, Mike. 2005. The Monster at Our Door: The Global Threat of Avian Flu. New York: Owl Books.
de Silva, A. M., K. R. Walder, T. J. Aitman, T. Gotoda, A. P. Goldstone, A. M. Hodge, M. P. de Courten, P. Z. Zimmet, and G. R. Collier. 1999. “Combination of Polymophisms in OB-R and the OB Gene Associated with Insulin Resistance in Nauruan Males.” International Journal of Obesity 23 (8): 816–822.
Harper, Kristin, and George Armelagos. 2010. “The Changing Disease-Scape in the Third Epidemiological Transition.” International Journal of Environmental Research and Public Health 7 (2): 675–697.
Harris, Marvin. 1989. “Life Without Chiefs.” New Age Journal, November/December: 42–45, 205–209.
International Diabetes Federation (IDF). 2018. IDF Diabetes Atlas. Eighth Edition. www.diabetesatlas.org/key-messages.html.
Jain, H. K.. 2012. “Transition to Twenty-First Century Agriculture: Change of Direction.” Agricultural Research 1 (1): 12–17.
Jones, Kate E., Nikkita G. Patel, Mark A. Levy, Adam Storeygard, Deborah Balk, John L. Gittleman, and Peter Daszak. 2008. “Global Trends in Emerging Infectious Disease.” Nature 451 (7181): 990–993.
Larsen, Clark Spencer. 2014. “Foraging to Farming Transition: Global Health Impacts, Trends, and Variation.” In Encyclopedia of Global Archaeology, edited by Claire Smith, 2818–2824. New York: Springer.
Leontis, Lisa M. N.d. “Type 2 Diabetes and Exercise: Exercise Makes It Easier to Control Your Diabetes.” https://www.endocrineweb.com/conditi...betes-exercise.
Lieberman, Leslie Sue. 2006. “Evolutionary and Anthropological Perspectives on Optimal Foraging in Obesogenic Environments.” Appetite 47 (1): 3–9.
Lucock, Mark D., Charlotte E. Martin, Zoe R. Yates, and Martin Veysey. 2014. “Diet and Our Genetic Legacy in the Recent Anthropocene: A Darwinian Perspective to Nutritional Health.” Journal of Evidence-Based Complementary and Alternative Medicine 19 (1): 68–83.
Marciniak, Stephanie, and George H. Perry. 2017. “Harnessing Ancient Genomes to Study the History of Human Adaptation.” Nature Reviews Genetics 18: 659–674.
Marmot, Michael. 2005. “Social Determinants of Health Inequality.” The Lancet 365 (9464): 1099–1104.
Martini, Frederic H., William C. Ober, Edwin F. Bartholomew, and Judi L. Nath. 2013. Visual Essentials of Anatomy & Physiology. Boston, MA: Pearson.
McKee, Trudy, and James R. McKee. 2015. Biochemistry: The Molecular Basis of Life. Sixth Edition. Oxford, UK: Oxford University Press.
Moss, Michael. 2013. Salt, Sugar, Fat: How the Food Giants Hooked Us. New York: Random House.
National Institutes of Health (NIH). 2017. “Obesity and Cancer Fact Sheet.” Last modified January, 2017. https://www.cancer.gov/about-cancer/...ity-fact-sheet.
Neel, James V. 1962. “Diabetes Mellitus: A ‘Thrifty’ Genotype Rendered Detrimental by ‘Progress’?” American Journal of Human Genetics 14 (4): 353–362.
O’Keefe Osborn, Corinne. 2017. “Type 1 and Type 2 Diabetes: What’s the Difference?” Healthline Newsletter, August 24. www.healthline.com/health/Di...ype-2-diabetes.
Omran, Abdel R. 1971. “The Epidemiological Transition: A Theory of the Epidemiology of Population Change.” Milbank Memorial Fund Quarterly 49 (4): 509–538.
Omran, Abdel R. 2005. “The Epidemiological Transition: A Theory of the Epidemiology of Population Change.” The Milbank Quarterly 83 (4): 731–757.
Physical Activity Council. 2018. 2018 Participation Report. www.physicalactivitycouncil.c...fs/current.pdf.
Pontzer, Herman, David A. Raichlen, Brian M. Wood, Audax Z. P. Mabulla, Susan B. Racette, and Frank W. Marlowe. 2012. “Hunter-Gatherer Energetics and Obesity.” PLoS ONE 7 (7): e40503. doi:10.1371/journal.pone.0040503.
Pritchard, Jonathan K. 2010. “How We Are Evolving.” Scientific American 303 (4): 4047.
Rankinen, Tuomo, Aamir Zuberi, Yvon C. Chagnon, S. John Weisnagel, George Argyropoulos, Brandon Walts, Louis Pérusse, and Claude Bouchard. 2006. “The Human Obesity Gene Map: The 2005 Update.” Obesity 14 (4): 529–644.
Smith-Morris, Carolyn M. 2004. “Reducing Diabetes in Indian Country: Lessons from the Three Domains Influencing Pima Diabetes.” Human Organization 63 (1): 34–46.
Stearns, Stephen C., Randolph M. Nesse, and David Haig. 2008. “Introducing Evolutionary Thinking into Medicine.” In Evolution in Health and Disease, edited by Stephen C. Stearns and Jacob C. Koella, 3–15. United Kingdom: Oxford University Press.
St. Pierre, Danielle. 2018. “The 15 Best Potato Chips for Every Flavor Craving.” Best, April 6. Retrieved June 13, 2018 from https://www.bestproducts.com/eats/fo...-potato-chips/.
Ventola, C. Lee. 2015. “The Antibiotic Resistance Crisis: Part I: Causes and Threats.” Pharmacy & Therapeutics 40 (4): 277–283.
Versini, M., Jeandel, P., Bashi, T., Bizzaro, G., Blank, M., and Shoenfeld, Y. 2015. “Unraveling the Hygiene Hypothesis of Helminthes and Autoimmunity: Origins, Pathophysiology, and Clinical Applications.” BMC Medicine, 13: 81. https://doi.org/10.1186/s12916-015-0306-7.
Vucenik, Ivana, and Joseph P. Stains. 2012. “Obesity and Cancer Risk: Evidence, Mechanisms, and Recommendations.” Special issue, “Nutrition and Physical Activity in Aging, Obesity, and Cancer,” Annals of the New York Academy of Sciences Volume 1271:: 37–43.
World Health Organization (WHO). 2016. Global Report on Diabetes. http://apps.who.int/iris/bitstream/h...565257_eng.pdf.
World Health Organization (WHO). 2017b. “Obesity and Overweight.” Fact Sheet. Last modified October 2017. http://www.who.int/mediacentre/factsheets/fs311/en/.
World Health Organization (WHO). n.d. “Influenza.” Accessed January 7, 2019 from https://www.who.int/influenza/human_...earch/faqs/en/.
Worthman, Carol M., and Jennifer Kuzara. 2005. “Life History and the Early Origins of Health Differentials.” American Journal of Human Biology 17 (1): 95–112.
Zuckerman, Molly K., and George J. Armelagos. 2014. “The Hygiene Hypothesis and the Second Epidemiologic Transition.” In Modern Environments and Human Health: Revisiting the Second Epidemiologic Transition, edited by Molly K. Zuckerman, 301-320. Hoboken, NJ: Wiley-Blackwell.
FIGURE ATTRIBUTIONS
Figure \(\PageIndex{1}\): Obesity rates by country original to Explorations: An Open Invitation to Biological Anthropology by Katie Nelson is under a CC BY-NC 4.0 License. Based on data from Obesity Update. 2017. Organisation for Economic Co-operation and Development (OECD) Health Statistics.
Figure \{\PageIndex{2}\} Participants of a walk against Diabetes and for general fitness around Nauru airport by Lorrie Graham, Department of Foreign Affairs and Trade is used under a CC BY 2.0 License.
Figure \{PageIndex{3}\} Medical complications of obesity by the Centers for Disease Control and Prevention (CDC) is in the public domain.
Figure \{\PageIndex{4}\} Glucose metabolism original to Explorations: An Open Invitation to Biological Anthropology by Mary Nelson is under a CC BY-NC 4.0 License.
Figure \{\PageIndex{5}\} Type 1 and Type 2 Diabetes original to Explorations: An Open Invitation to Biological Anthropology by Mary Nelson is under a CC BY-NC 4.0 License.
TABLE ATTRIBUTIONS
Table \(\PageIndex{1}\) The potato in three modern forms a derivative work original to Explorations: An Open Invitation to Biological Anthropology by Joylin Namie and Katie Nelson is under a CC BY-NC 4.0 License. [Includes Potato by unknown, public domain (CC0); McDonalds-French-Fries-Plate by Evan-Amos, public domain (CC0); Potato chips bowl by unknown, public domain (CC0).]