
16.5: Are We Still Evolving?
- Page ID
- 177800
ARE WE STILL EVOLVING?
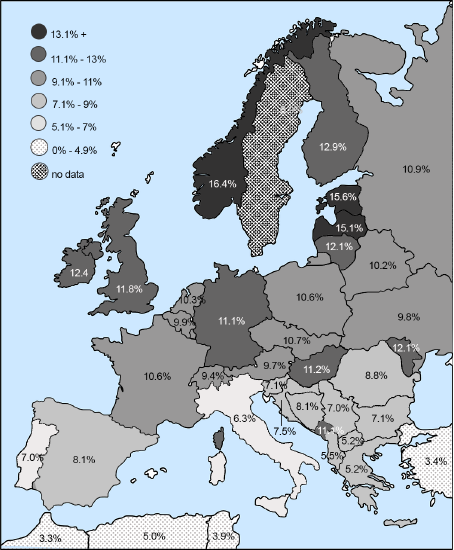 Figure \(\PageIndex{1}\): Map of CCR5-delta32 allele distribution.
Figure \(\PageIndex{1}\): Map of CCR5-delta32 allele distribution..png?revision=1&size=bestfit&width=843&height=500) Figure \(\PageIndex{2}\): Map of global HIV infection.
Figure \(\PageIndex{2}\): Map of global HIV infection.FOOD FOR THOUGHT
This chapter focused on health conditions prevalent in contemporary, industrialized societies that are due, in part, to the mismatch between our evolved biology and modern cultural and physical environments. Obesity is at the root of it all. Claude Bouchard (2007) identified factors contributing to the global epidemic of obesity and the diseases associated with it. These are the built environment and the social environment, which together form the obesogenic environment in which unhealthy behaviors are encouraged. This chapter will close by examining each of these in a college context.
 Figure \(\PageIndex{3}\): Students walking around campus.
Figure \(\PageIndex{3}\): Students walking around campus.In terms of the built environment, consider your campus or neighborhood from an evolutionary perspective. To what degree does the construction of the space lend itself to physical activity as part of daily life? Is your campus constructed in such a way that it promotes the use of automobiles at the expense of walking or biking? If driving is necessary, is parking available close to the buildings or do you need to walk a fair distance from the parking lot to your destination? Do the buildings have stairs or ramps or is it necessary to take the elevator? Is it possible to negotiate safely around campus or the neighborhood on foot or by bike in all weather? After dark? How about the classrooms and computer labs? Do they have standing or treadmill desks as options? Does your class schedule encourage walking from building to building between classes, or are most courses in your major scheduled in the same location? I regularly have students who sit in the same room for hours, not even changing desks, while instructors rush from place to place. Most college majors also lack a physical activity requirement, leaving it up to students to incorporate exercise into already-busy schedules (See Figure \(\PageIndex{3}\)).
Sociocultural factors that contribute to obesity include food advertising, ubiquitous fast-food and junk food options, and social pressure to consume, all of which are present on college campuses. Although nutritional options on campuses have improved in recent years, many students find eating healthy in the dining halls and dorms challenging (Plotnikoff et al. 2015), and students who live off campus fare even worse (Small et al. 2013). There are also parties and other social events, a normal part of college life, that often involve unhealthy food and encourage behaviors like alcohol consumption and smoking. Give some thought to the social atmosphere on your campus and the ways in which it may contribute to obesity. My own freshman orientation involved a succession of pizza parties, ice cream socials, and barbecues, followed by late-night runs to the nearest fast-food outlet. The purpose of these events was to encourage people to make friends and feel comfortable living away from home, but the foods served were not healthy, and there was social pressure to join in and be part of the group. Such activities set students up for the “freshman fifteen” and then some. They also reinforce the idea that being social involves eating (and sometimes drinking and/or smoking).
Sedentarism and inactivity are also built into the academics of college life. Digital technology is a significant contributor to obesity. Students use laptops and cell phones to take notes, complete their work outside of class, and access social media. There are also video games, virtual reality headsets, and streaming television and movies for entertainment. The built environment of college already necessitates that students sit in class for hours each day, then sit at computers to complete work outside of class. The social environment enabled by digital technology encourages sitting around for entertainment. It is telling that we call it “binge watching” when we spend hours watching our favorite shows. Doing so often involves eating, as well as multiple exposures to food advertising embedded in the shows themselves. In these many ways, college contributes to the development of obesogenic behaviors that can have negative health ramifications long after college is over (Small et al. 2013).
In the U.S., the greatest increase in obesity is among young adults aged 18–29 years, a significant percentage of whom are college students (Plotnikoff et al. 2015). Analyses of college students’ behavior across semesters shows consumption of fruits and vegetables drops over time, as does the amount of physical activity, while consumption of sugar-sweetened beverages and fast-food goes up, leading to weight gain at nearly six times the rate of the general public (Small et al. 2013). Realizing this, many colleges and universities have instituted programs to encourage healthier eating and more physical activity among students (Plotnikoff et al. 2015). Some schools have even done away with collegiate sports, which often serve a small percentage of students, in favor of campus-wide efforts at getting everyone active (Tierney 2013). Investigate the options on your campus and take advantage of opportunities. We cannot change our biology, but we can certainly change our habits.
REFERENCES
Andrews, Tessa M., Steven T. Kalinowski, and Mary J. Leonard. 2011. “Are Humans Evolving? A Classroom Discussion to Change Students’ Misconceptions Regarding Natural Selection.” Evolution: Education and Outreach 4 (3): 456–466.
Bouchard, Claude. 2007. “The Biological Predisposition to Obesity: Beyond the Thrifty Genotype Scenario.” International Journal of Obesity 31: 1337–1339.
Crow, James F., and Motoo Kimura. 1970. An Introduction to Population Genetics Theory. New York: Harper and Row.
Devuyst, Olivier. 2014. “High Time for Human Height.” Peritoneal Dialysis International 34 (7): 685–686.
Gladwell, Malcolm. 2007. Blink: The Power of Thinking Without Thinking. New York: Back Bay Books.
Goulder, Philip J., Sharon R. Lewin, and Ellen M. Leitman. 2016. “Paediatric HIV Infection: The Potential for Cure.” Nature Reviews Immunology 16: 259–271.
Guadagno, Rosanna E., Bradley M. Okdie, and Sara A. Kruse. 2012. “Dating Deception: Gender, Online Dating, and Exaggerated Self-Presentation.” Computers in Human Behavior 28 (2): 642–647.
Hatton, Tim. 2014. “Why Did Humans Grow Four Inches in 100 Years? It Wasn’t Just Diet.” The Conversation, May 1. https://theconversation.com/why-did-...ust-diet-25919.
Hays, J. N. 2005. Epidemics and Pandemics: Their Impacts on Human History. Santa Barbara, CA: ABC-CLIO, Inc.
Lopalco, Lucia. 2010. “CCR5: From Natural Resistance to a New Anti-HIV Strategy.” Viruses 2 (2): 574–600.
Main, Douglas. 2013. “Ancient Mutation Explains Missing Wisdom Teeth.” Live Science, March 13. https://www.livescience.com/27529-mi...dom-teeth.html.
Novembre, John, Alison P. Galvani, and Montgomery Slatkin. 2005. “The Geographic Spread of the CCR5 Δ32 HIV-Resistance Allele.” PLoS Biology 3 (11): e339.
Pamuk, Şevket. 2007. “The Black Death and the Origins of the ‘Great Divergence’ across Europe, 1300–1600.” European Review of Economic History 11 (3): 289–317.
Plotnikoff, Ronald C., Sarah A. Costigan, Rebecca L. Williams, Melinda J. Hutchesson, Sarah G. Kennedy, Sara L. Robards, Jennifer Allen, Clare E. Collins, Robin Callister, and John Germov. 2015. “Effectiveness of Interventions Targeting Physical Activity, Nutrition and Healthy Weight for University and College Students: A Systematic Review and Meta-analysis.” International Journal of Behavioral Nutrition and Physical Activity 12 (1): 1–10.
Sharp, Paul M., and Beatrice H. Hahn. 2011. “Origins of HIV and the AIDS Pandemic.” Cold Springs Harbor Perspectives in Medicine 1 (1): a006841.
Small, Meg, Lisa Bailey-Davis, Nicole Morgan, and Jennifer Maggs. 2013. “Changes in Eating and Physical Activity Behaviors across Seven Semesters of College: Living On or Off Campus Matters.” Health Education and Behavior 40 (4): 435–441.
Stearns, Stephen C., Randolph M. Nesse, and David Haig. 2008. “Introducing Evolutionary Thinking into Medicine.” In Evolution in Health and Disease, edited by Stephen C. Stearns and Jacob C. Koella, 3–15. United Kingdom: Oxford University Press.
Tierney, Mike. 2013. “At Spelman, Dropping Sports in Favor of Fitness.” New York Times, April 13. https://www.nytimes.com/2013/04/14/s...f-fitness.html.
UNAIDS. 2018. “Fact Sheet: Latest Statistics on the AIDS Epidemic.” www.unaids.org/en/resources/fact-sheet.
FIGURE ATTRIBUTIONS
Figure \(\PageIndex{1}\) Map of CCR5-delta32 allele distribution original to Explorations: An Open Invitation to Biological Anthropology by Katie Nelson is under a CC BY-NC 4.0 License. [Includes Europe Map Western Political 32847, unknown, Pixabay License; data from Solloch, Ute V., Kathrin Lang, Vinzenz Lange, and Irena Böhme. 2017. “Frequencies of gene variant CCR5-Δ32 in 87 countries based on next-generation sequencing of 1.3 million individuals sampled from 3 national DKMS donor centers.” Human Immonology, 78 (11-12).]
Figure \(\PageIndex{2}\) HIV-world-map-UNAIDS by UNAIDS has been designated to the public domain (CC0).
Figure \(\PageIndex{3}\) Row four man woman people walking together 3755342 by MaxPixel has been designated to the public domain (CC0).