
15.10: Disorders in Childhood
- Page ID
- 200509

\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\(\newcommand{\avec}{\mathbf a}\) \(\newcommand{\bvec}{\mathbf b}\) \(\newcommand{\cvec}{\mathbf c}\) \(\newcommand{\dvec}{\mathbf d}\) \(\newcommand{\dtil}{\widetilde{\mathbf d}}\) \(\newcommand{\evec}{\mathbf e}\) \(\newcommand{\fvec}{\mathbf f}\) \(\newcommand{\nvec}{\mathbf n}\) \(\newcommand{\pvec}{\mathbf p}\) \(\newcommand{\qvec}{\mathbf q}\) \(\newcommand{\svec}{\mathbf s}\) \(\newcommand{\tvec}{\mathbf t}\) \(\newcommand{\uvec}{\mathbf u}\) \(\newcommand{\vvec}{\mathbf v}\) \(\newcommand{\wvec}{\mathbf w}\) \(\newcommand{\xvec}{\mathbf x}\) \(\newcommand{\yvec}{\mathbf y}\) \(\newcommand{\zvec}{\mathbf z}\) \(\newcommand{\rvec}{\mathbf r}\) \(\newcommand{\mvec}{\mathbf m}\) \(\newcommand{\zerovec}{\mathbf 0}\) \(\newcommand{\onevec}{\mathbf 1}\) \(\newcommand{\real}{\mathbb R}\) \(\newcommand{\twovec}[2]{\left[\begin{array}{r}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\ctwovec}[2]{\left[\begin{array}{c}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\threevec}[3]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\cthreevec}[3]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\fourvec}[4]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\cfourvec}[4]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\fivevec}[5]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\cfivevec}[5]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\mattwo}[4]{\left[\begin{array}{rr}#1 \amp #2 \\ #3 \amp #4 \\ \end{array}\right]}\) \(\newcommand{\laspan}[1]{\text{Span}\{#1\}}\) \(\newcommand{\bcal}{\cal B}\) \(\newcommand{\ccal}{\cal C}\) \(\newcommand{\scal}{\cal S}\) \(\newcommand{\wcal}{\cal W}\) \(\newcommand{\ecal}{\cal E}\) \(\newcommand{\coords}[2]{\left\{#1\right\}_{#2}}\) \(\newcommand{\gray}[1]{\color{gray}{#1}}\) \(\newcommand{\lgray}[1]{\color{lightgray}{#1}}\) \(\newcommand{\rank}{\operatorname{rank}}\) \(\newcommand{\row}{\text{Row}}\) \(\newcommand{\col}{\text{Col}}\) \(\renewcommand{\row}{\text{Row}}\) \(\newcommand{\nul}{\text{Nul}}\) \(\newcommand{\var}{\text{Var}}\) \(\newcommand{\corr}{\text{corr}}\) \(\newcommand{\len}[1]{\left|#1\right|}\) \(\newcommand{\bbar}{\overline{\bvec}}\) \(\newcommand{\bhat}{\widehat{\bvec}}\) \(\newcommand{\bperp}{\bvec^\perp}\) \(\newcommand{\xhat}{\widehat{\xvec}}\) \(\newcommand{\vhat}{\widehat{\vvec}}\) \(\newcommand{\uhat}{\widehat{\uvec}}\) \(\newcommand{\what}{\widehat{\wvec}}\) \(\newcommand{\Sighat}{\widehat{\Sigma}}\) \(\newcommand{\lt}{<}\) \(\newcommand{\gt}{>}\) \(\newcommand{\amp}{&}\) \(\definecolor{fillinmathshade}{gray}{0.9}\)Attention Deficit/Hyperactivity Disorder
Diego is always active, from the time he wakes up in the morning until the time he goes to bed at night. His mother reports that he came out the womb kicking and screaming, and he has not stopped moving since. He has a sweet disposition, but always seems to be in trouble with his teachers, parents, and after-school program counselors. He seems to accidentally break things; he lost his jacket three times last winter, and he never seems to sit still. His teachers believe he is a smart child, but he never finishes anything he starts and is so impulsive that he does not seem to learn much in school.
Diego likely has attention deficit/hyperactivity disorder (ADHD). The symptoms of this disorder were first described by Hans Hoffman in the 1920s. While taking care of his son while his wife was in the hospital giving birth to a second child, Hoffman noticed that the boy had trouble concentrating on his homework, had a short attention span, and had to repeatedly go over easy homework to learn the material (Jellinek & Herzog, 1999). Later, it was discovered that many hyperactive children—those who are fidgety, restless, socially disruptive, and have trouble with impulse control—also display short attention spans, problems with concentration, and distractibility. By the 1970s, it had become clear that many children who display attention problems often also exhibit signs of hyperactivity. In recognition of such findings, the DSM-III (published in 1980) included a new disorder: attention deficit disorder with and without hyperactivity, now known as attention deficit/hyperactivity disorder (ADHD).
A child with ADHD shows a constant pattern of inattention and/or hyperactive and impulsive behavior that interferes with normal functioning (APA, 2013). Some of the signs of inattention include great difficulty with and avoidance of tasks that require sustained attention (such as conversations or reading), failure to follow instructions (often resulting in failure to complete school work and other duties), disorganization (difficulty keeping things in order, poor time management, sloppy and messy work), lack of attention to detail, becoming easily distracted, and forgetfulness. Hyperactivity is characterized by excessive movement, and includes fidgeting or squirming, leaving one’s seat in situations when remaining seated is expected, having trouble sitting still (e.g., in a restaurant), running about and climbing on things, blurting out responses before another person’s question or statement has been completed, difficulty waiting one’s turn for something, and interrupting and intruding on others. Frequently, the hyperactive child comes across as noisy and boisterous. The child’s behavior is hasty, impulsive, and seems to occur without much forethought; these characteristics may explain why adolescents and young adults diagnosed with ADHD receive more traffic tickets and have more automobile accidents than do others (Thompson, Molina, Pelham, & Gnagy, 2007).
ADHD occurs in about 8% of children (Danielson et al, 2016), and studies estimate that for about 60% of these people, ADHD continues into adulthood (Sibley et al 2016). On the average, boys are 3 times more likely to have ADHD than are girls; however, such findings might reflect the greater propensity of boys to engage in aggressive and antisocial behavior and thus incur a greater likelihood of being referred to psychological clinics (Barkley, 2006). Children with ADHD face severe academic and social challenges. Compared to their non-ADHD counterparts, children with ADHD have lower grades and standardized test scores and higher rates of expulsion, grade retention, and dropping out (Loe & Feldman, 2007). they also are less well-liked and more often rejected by their peers (Hoza et al., 2005).
A recent study found that nearly 81% of those whose ADHD persisted into adulthood had experienced at least one other comorbid disorder, compared to 47% of those whose ADHD did not persist (Barbaresi et al., 2013).
Life Problems from ADHD
Children with ADHD face considerably worse long-term outcomes than do those children who do not have ADHD. Adults diagnosed with ADHD in childhood, but not treated for ADHD, have been reported to have poor outcomes in a wide range of areas of life, including social function, education, criminality, alcohol use, substance use, and occupational outcomes (Arnold et al, 2015). In one investigation, 135 adults who had been identified as having ADHD symptoms in the 1970s were contacted decades later and interviewed (Klein et al., 2012). Compared to a control sample of 136 participants who had never been diagnosed with ADHD, those who were diagnosed as children:
Longitudinal studies also show that children diagnosed with ADHD are at higher risk for substance abuse problems. One study reported that childhood ADHD predicted later drinking problems, daily smoking, and use of marijuana and other illicit drugs (Molina & Pelham, 2003). The risk of substance abuse problems appears to be even greater for those with ADHD who also exhibit antisocial tendencies (Marshal & Molina, 2006).
Diagnosis, treatment, and general awareness of ADHD has certainly improved in the decades since the people in the above studies were diagnosed. Studies that include more recent outcomes show positive effects of treatment as opposed to non-treatment (Harpin, 2013; Arnold 2015). In most cases, the same studies indicate that more research and work needs to be undertaken to understand the most effect treatments and their impacts.
Causes of ADHD
Family and twin studies indicate that genetics play a significant role in the development of ADHD. Burt (2009), in a review of 26 studies, reported that the median rate of concordance for identical twins was .66 (one study reported a rate of .90), whereas the median concordance rate for fraternal twins was .20. This study also found that the median concordance rate for unrelated (adoptive) siblings was .09; although this number is small, it is greater than 0, thus suggesting that the environment may have at least some influence. Another review of studies concluded that the heritability of inattention and hyperactivity were 71% and 73%, respectively (Nikolas & Burt, 2010).
The specific genes involved in ADHD are thought to include at least two that are important in the regulation of the neurotransmitter dopamine (Gizer, Ficks, & Waldman, 2009), suggesting that dopamine may be important in ADHD. Indeed, medications used in the treatment of ADHD, such as methylphenidate (Ritalin) and amphetamine with dextroamphetamine (Adderall), have stimulant qualities and elevate dopamine activity. People with ADHD show less dopamine activity in key regions of the brain, especially those associated with motivation and reward (Volkow et al., 2009), which provides support to the theory that dopamine deficits may be a vital factor in the development this disorder (Swanson et al., 2007).
Brain imaging studies have shown that children with ADHD exhibit abnormalities in their frontal lobes, an area in which dopamine is in abundance. Compared to children without ADHD, those with ADHD appear to have smaller frontal lobe volume, and they show less frontal lobe activation when performing mental tasks. Recall that one of the functions of the frontal lobes is to inhibit our behavior. Thus, abnormalities in this region may go a long way toward explaining the hyperactive, uncontrolled behavior of ADHD.
By the 1970s, many had become aware of the connection between nutritional factors and childhood behavior. At the time, much of the public believed that hyperactivity was caused by sugar and food additives, such as artificial coloring and flavoring. Undoubtedly, part of the appeal of this hypothesis was that it provided a simple explanation of (and treatment for) behavioral problems in children. A statistical review of 16 studies, however, concluded that sugar consumption has no effect at all on the behavioral and cognitive performance of children (Wolraich, Wilson, & White, 1995). Additionally, although food additives have been shown to increase hyperactivity in non-ADHD children, the effect is rather small (McCann et al., 2007). Numerous studies, however, have shown a significant relationship between exposure to nicotine in cigarette smoke during the prenatal period and ADHD (Linnet et al., 2003). Maternal smoking during pregnancy is associated with the development of more severe symptoms of the disorder (Thakur et al., 2013).
Is ADHD caused by poor parenting? No. Remember, the genetics studies discussed above suggested that the family environment does not seem to play much of a role in the development of this disorder; if it did, we would expect the concordance rates to be higher for fraternal twins and adoptive siblings than has been demonstrated. All things considered, the evidence seems to point to the conclusion that ADHD is triggered more by genetic and neurological factors and less by social or environmental ones.
Many people believe that the rates of ADHD have increased in recent years, and there is evidence to support this contention. In a recent study, investigators found that the parent-reported prevalence of ADHD among children (4–17 years old) in the United States increased by 22% during a 4-year period, from 7.8% in 2003 to 9.5% in 2007 (CDC, 2010). Over time this increase in parent-reported ADHD was observed in all sociodemographic groups and was reflected by substantial increases in 12 states (Indiana, North Carolina, and Colorado were the top three). The increases were greatest for older teens (ages 15–17), multiracial and Hispanic children, and children with a primary language other than English. Another investigation found that from 1998–2000 through 2007–2009 the parent-reported prevalence of ADHD increased among U.S. children between the ages of 5–17 years old, from 6.9% to 9.0% (Akinbami, Liu, Pastor, & Reuben, 2011).
A major weakness of both studies was that children were not actually given a formal diagnosis. Instead, parents were simply asked whether or not a doctor or other health-care provider had ever told them their child had ADHD; the reported prevalence rates thus may have been affected by the accuracy of parental memory. Nevertheless, the findings from these studies raise important questions concerning what appears to be a demonstrable rise in the prevalence of ADHD. Although the reasons underlying this apparent increase in the rates of ADHD over time are poorly understood and, at best, speculative, several explanations are viable:
Autism Spectrum Disorder
A seminal paper published in 1943 by psychiatrist Leo Kanner described an unusual neurodevelopmental condition he observed in a group of children. He called this condition early infantile autism, and it was characterized mainly by an inability to form close emotional ties with others, speech and language abnormalities, repetitive behaviors, and an intolerance of minor changes in the environment and in normal routines (Bregman, 2005). What the DSM-5 refers to as autism spectrum disorder today, is a direct extension of Kanner’s work.
Autism spectrum disorder is probably the most misunderstood of the neurodevelopmental disorders. Children with this disorder show signs of significant disturbances in three main areas: (a) deficits in social interaction, (b) deficits in communication, and (c) repetitive patterns of behavior or interests. These disturbances appear early in life and cause serious impairments in functioning (APA, 2013). The child with autism spectrum disorder might exhibit deficits in social interaction by not initiating conversations with other children or turning their head away when spoken to. Typically, these children do not make eye contact with others and seem to prefer playing alone rather than with others. In some cases, it is almost as though these individuals live in a personal and isolated social world others are simply not privy to or able to penetrate. Communication deficits can range from a complete lack of speech, to one word responses (e.g., saying “Yes” or “No” when replying to questions or statements that require additional elaboration), to echoed speech (e.g., parroting what another person says, either immediately or several hours or even days later), to difficulty maintaining a conversation because of an inability to reciprocate others’ comments. These deficits can also include problems in using and understanding nonverbal cues (e.g., facial expressions, gestures, and postures) that facilitate normal communication.
Repetitive patterns of behavior or interests can be exhibited a number of ways. The child might engage in stereotyped, repetitive movements (rocking, head-banging, or repeatedly dropping an object and then picking it up), or they might show great distress at small changes in routine or the environment. In some cases, the person with autism spectrum disorder might show highly restricted and fixated interests that appear to be abnormal in their intensity. For instance, the person might learn and memorize every detail about something even though doing so serves no apparent purpose. Importantly, autism spectrum disorder is not the same thing as intellectual disability, although these two conditions are often comorbid. The DSM-5 specifies that the symptoms of autism spectrum disorder are not caused or explained by intellectual disability.
Life Problems From Autism Spectrum Disorder
Autism spectrum disorder is referred to in everyday language as autism; in fact, the disorder was termed “autistic disorder” in earlier editions of the DSM, and its diagnostic criteria were much narrower than those of autism spectrum disorder. The qualifier “spectrum” in autism spectrum disorder is used to indicate that individuals with the disorder can show a range, or spectrum, of symptoms that vary in their magnitude and severity: some severe, others less severe. The previous edition of the DSM included a diagnosis of Asperger’s disorder, generally recognized as a less severe form of autistic disorder; individuals diagnosed with Asperger’s disorder were described as having average or high intelligence and a strong vocabulary, but exhibiting impairments in social interaction and social communication, such as talking only about their special interests (Wing, Gould, & Gillberg, 2011). However, because research has failed to demonstrate that Asperger’s disorder differs qualitatively from autistic disorder, the DSM-5 does not include it, which is prompting concerns among some parents that their children may no longer be eligible for special services (“Asperger’s Syndrome Dropped,” 2012). Some individuals with autism spectrum disorder, particularly those with better language and intellectual skills, can live and work independently as adults. However, most do not because the symptoms remain sufficient to cause serious impairment in many realms of life (APA, 2013).
Current estimates from the Center for Disease Control and Prevention’s Autism and Developmental Disabilities Monitoring Network indicate that 1 in 59 children in the United States has autism spectrum disorder; the disorder is 4 times more common among boys (1 in 38) than in girls (1 in 152) (Baio et al, 2018). Rates of autistic spectrum disorder have increased dramatically since the 1980s. For example, California saw an increase of 273% in reported cases from 1987 through 1998 (Byrd, 2002); between 2000 and 2008, the rate of autism diagnoses in the United States increased 78% (CDC, 2012). Although it is difficult to interpret this increase, it is possible that the rise in prevalence is the result of the broadening of the diagnosis, increased efforts to identify cases in the community, and greater awareness and acceptance of the diagnosis. In addition, mental health professionals are now more knowledgeable about autism spectrum disorder and are better equipped to make the diagnosis, even in subtle cases (Novella, 2008).
Causes of Autism Spectrum Disorder
The exact causes of autism spectrum disorder remain unknown despite massive research efforts over the last two decades (Meek, Lemery-Chalfant, Jahromi, & Valiente, 2013). Autism appears to be strongly influenced by genetics, as identical twins show concordance rates of 60%–90%, whereas concordance rates for fraternal twins and siblings are 5%–10% (Autism Genome Project Consortium, 2007). Many different genes and gene mutations have been implicated in autism (Meek et al., 2013). Among the genes involved are those important in the formation of synaptic circuits that facilitate communication between different areas of the brain (Gauthier et al., 2011). A number of environmental factors are also thought to be associated with increased risk for autism spectrum disorder, at least in part, because they contribute to new mutations. These factors include exposure to pollutants, such as plant emissions and mercury, urban versus rural residence, and vitamin D deficiency (Kinney, Barch, Chayka, Napoleon, & Munir, 2009).
Child Vaccinations and Autism Spectrum Disorder
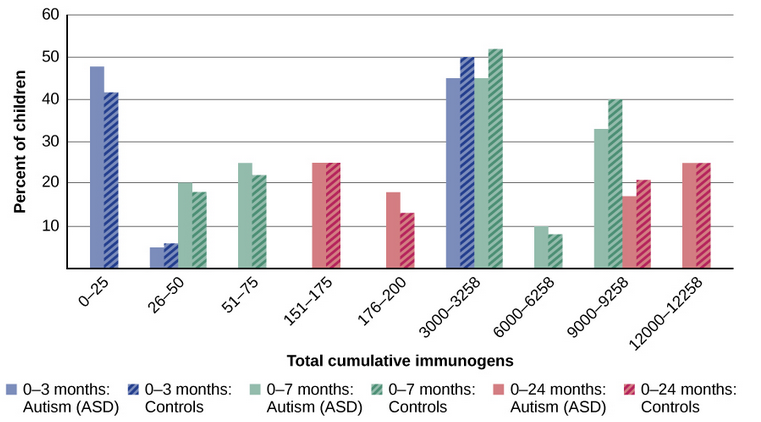
In the late 1990s, a prestigious medical journal published an article purportedly showing that autism is triggered by the MMR (measles, mumps, and rubella) vaccine. These findings were very controversial and drew a great deal of attention, sparking an international forum on whether children should be vaccinated. In a shocking turn of events, some years later the article was retracted by the journal that had published it after evidence of fraud and unethical practices on the part of the lead researcher. Despite the retraction, the reporting in popular media led to concerns about a possible link between vaccines and autism persisting. A recent survey of parents, for example, found that roughly a third of respondents expressed such a concern (Kennedy, LaVail, Nowak, Basket, & Landry, 2011); and perhaps fearing that their children would develop autism, more than 10% of parents of young children refuse or delay vaccinations (Dempsey et al., 2011). Some parents of children with autism mounted a campaign against scientists who refuted the vaccine-autism link. Even politicians and several well-known celebrities weighed in; for example, actress Jenny McCarthy (who believed that a vaccination caused her son’s autism) co-authored a book on the matter. However, there is no scientific evidence that a link exists between autism and vaccinations (Hughes, 2007). Indeed, a recent study compared the vaccination histories of 256 children with autism spectrum disorder with that of 752 control children across three time periods during their first two years of life (birth to 3 months, birth to 7 months, and birth to 2 years) (DeStefano, Price, & Weintraub, 2013). At the time of the study, the children were between 6 and 13 years old, and their prior vaccination records were obtained. Because vaccines contain immunogens (substances that fight infections), the investigators examined medical records to see how many immunogens children received to determine if those children who received more immunogens were at greater risk for developing autism spectrum disorder. The results of this study, a portion of which are shown in Figure 15.19, clearly demonstrate that the quantity of immunogens from vaccines received during the first two years of life were not at all related to the development of autism spectrum disorder. There is not a relationship between vaccinations and autism spectrum disorders.
Why does concern over vaccines and autism spectrum disorder persist? Since the proliferation of the Internet in the 1990s, parents have been constantly bombarded with online information that can become magnified and take on a life of its own. The enormous volume of electronic information pertaining to autism spectrum disorder, combined with how difficult it can be to grasp complex scientific concepts, can make separating good research from bad challenging (Downs, 2008). Notably, the study that fueled the controversy reported that 8 out of 12 children—according to their parents—developed symptoms consistent with autism spectrum disorder shortly after receiving a vaccination. To conclude that vaccines cause autism spectrum disorder on this basis, as many did, is clearly incorrect for a number of reasons, not the least of which is because correlation does not imply causation, as you’ve learned.
Additionally, as was the case with diet and ADHD in the 1970s, the notion that autism spectrum disorder is caused by vaccinations is appealing to some because it provides a simple explanation for this condition. Like all disorders, however, there are no simple explanations for autism spectrum disorder. Although the research discussed above has shed some light on its causes, science is still a long way from complete understanding of the disorder.