Cancer is the second-leading cause of death globally, causing one in every six deaths and killing nearly nine million people in 2015 (WHO 2018). Lifetime cancer risk in developed Western populations is now one in two, or 50% (Greaves 2015). Approximately one-third of deaths from cancer are due to behavioral and dietary factors, including high body mass index (BMI), low fruit and vegetable intake, lack of physical activity, and the use of tobacco and alcohol. Depending on the type of cancer and one’s own genetic inheritance, these factors can increase cancer risk from 2- to 100-fold (Greaves 2015). Cancer is the result of interactions between a person’s genes and three categories of external agents: physical carcinogens (e.g., ultraviolet radiation), chemical carcinogens (e.g., tobacco smoke, asbestos), and biological carcinogens, such as infections from certain viruses, bacteria, or parasites (WHO 2018). Obesity is also a risk factor for cancer, including of the breast, endometrium, kidney, colon, esophagus, stomach, pancreas, and gallbladder (National Institutes of Health 2017; Vucenik and Stains 2012).
Cancer has been regarded as a relatively recent affliction for humans that became a problem after we were exposed to modern carcinogens and lived long enough to express the disease (David and Zimmerman 2010). Given the long history that humans share with many oncogenic (cancer-causing) parasites and viruses (Ewald 2018), and the recent discovery of cancer in the metatarsal bone of a 1.8-million-year-old hominin (Odes et al. 2016), this view is being challenged (See “Special Topic: Life Choices and Reproductive Cancers in Women”). The difficulties of identifying cancer in archaeological populations are many. Most cancer occurs in soft tissue, which rarely preserves, and fast-growing cancers would likely kill victims before leaving evidence in bone. It is also difficult to distinguish cancer from benign growths and inflammatory disease in ancient fossils, and there is often postmortem damage to fossil evidence from scavenging and erosion. However, using 3-D images, South African researchers recently diagnosed a type of cancer called osteosarcoma in a toe bone belonging to a human relative who died in Swartkrans Cave between 1.6 and 1.8 million years ago (Randolph-Quinney et al. 2016). This study provides the earliest evidence of cancer in hominins.
Special Topic: Life Choices and Reproductive Cancers in Women
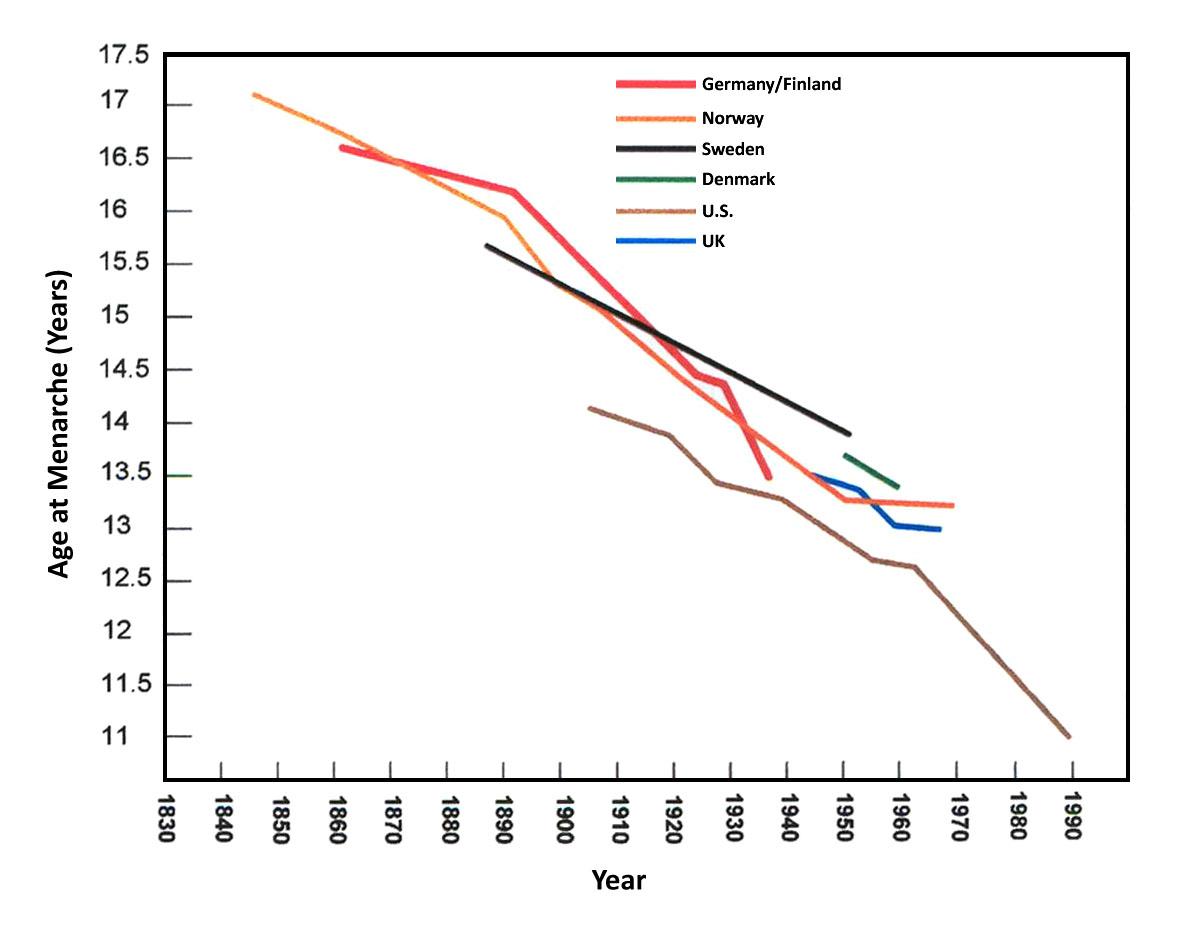
Behavioral or “lifestyle” choices have an impact on cancer risk. Breast cancer is one example. It is the most common cancer in women worldwide, but incidence of new cases varies from 19.3 per 100,000 women in Eastern Africa to 89.7 per 100,000 women in Western Europe (WHO 2018). These differences are attributable to cultural changes among women in Western, industrialized countries that are a mismatch for our evolved reproductive biology. Age at menarche, the onset of menstrual periods, has dropped over the course of the last century from 16 to 12 years of age in the U.S. and Europe, with some girls getting their periods and developing breasts as young as eight years old (Greenspan and Deardorff 2014, Figure 16.10). A World Health Organization study involving 34 countries in Europe and North America suggests the primary reason for the increase in earlier puberty is obesity, with differences in BMI accounting for 40% of individual- and country-level variance (Currie et al. 2012). Early puberty in girls is associated with increased risk of breast cancer, ovarian cancer, diabetes, and high cholesterol in later life (Pierce and Hardy 2012).
At the same time that age at puberty is dropping for girls in Western nations, age at birth of the first child is later, at 26 years old (Mathews and Hamilton 2016). Women are also having fewer children, two on average (Gao 2015), with 15% of women choosing to remain childless (Livingston 2015). Rates of breastfeeding have risen in recent decades but drop to only 27% of infants once babies reach 12 months of age (CDC 2014). In contrast, data from modern foraging populations (Eaton et al. 1994) indicate that age at menarche is around 16 years old, age at birth of the first child is 19, breastfeeding on-demand continues for three years for each child, and the number of children averages six. These differences relate to elevated risk for reproductive cancers, including breast cancer, among women in developed countries.
Other than an established genetic risk (e.g., BRCA gene), the primary risk factor for breast cancer is exposure to estrogen. For women living in modern, industrialized economies, this exposure now often comes from women’s own ovaries rather than from external environmental sources (Stearns, Nesse, and Haig 2008). There is nothing biologically normal about regular monthly periods. Women in cultures without contraception are pregnant or breastfeeding for much of their reproductive lives, resulting in 100 or so menstrual cycles per lifetime. In contrast, Western women typically experience 400 or more (Strassmann 1997). This is partly due to early puberty. From menarche to the birth of a woman’s first child can be 14 years or longer in Western populations, after which breastfeeding, if undertaken at all, lasts for a few weeks or months. Oral contraceptives or other hormonal methods to control reproduction induce monthly periods. Age at menopause (the cessation of menstrual cycles) is 50–55 years old across human populations. For Western women, this translates into forty years of menstrual cycling. Each month the body prepares for a pregnancy that never occurs, experiencing cell divisions that put women at risk for cancers of the breast, endometrium, ovaries, and uterus (Strassmann 1999). Obesity adds to risk, as adipose (fat) tissues are the main source of estrogen biosynthesis. Thus, weight gain during the postmenopausal stage means higher exposure to estrogen and a greater risk of cancer (Ali 2014).
Women cannot return to our evolutionary past, and there are important social and economic reasons for delaying pregnancy and having fewer children. These include achieving educational and career goals, greater earning power, a reduction in the gender pay gap, more enduring marriages, and a decrease in the number of women needing public assistance (Sonfield et al. 2013). There are also cultural means by which we might reduce the risk of reproductive cancers. These include reformulating hormonal contraceptives with enough estrogen to maintain bone density but reducing the number of menstrual periods over the reproductive lifespan (Stearns, Nesse, and Haig 2008). Reducing fat intake may also lower estrogen levels. High-fat diets contribute to breast tumor development, while high fiber diets are beneficial in decreasing intestinal resorption of estrogenic hormones. Exercise also appears protective. Studies of former college athletes demonstrate risks of breast, uterine, and ovarian cancers later in life two to five times lower than those of nonathletes (Eaton et al. 1994).