Distinguish between psychotherapy and biomedical therapy
Recognize various orientations to psychotherapy
Discuss psychotropic medications and recognize which medications are used to treat specific psychological disorders
One of the goals of therapy is to help a person stop repeating and reenacting destructive patterns and to start looking for better solutions to difficult situations. This goal is reflected in the following poem:
Autobiography in Five Short Chapters by Portia Nelson (1993)
Chapter One
I walk down the street.
There is a deep hole in the sidewalk.
I fall in.
I am lost. . . . I am helpless.
It isn't my fault.
It takes forever to find a way out.
Chapter Two
I walk down the same street.
There is a deep hole in the sidewalk.
I pretend I don't see it.
I fall in again.
I can't believe I am in this same place.
But, it isn't my fault.
It still takes a long time to get out.
Chapter Three
I walk down the same street.
There is a deep hole in the sidewalk.
I see it is there.
I still fall in . . . it's a habit . . . but,
my eyes are open.
I know where I am.
It is my fault.
I get out immediately.
Chapter Four
I walk down the same street.
There is a deep hole in the sidewalk.
I walk around it.
Chapter Five
I walk down another street.
Two types of therapy are psychotherapy and biomedical therapy. Both types of treatment help people with psychological disorders, such as depression, anxiety, and schizophrenia. Psychotherapy is a psychological treatment that employs various methods to help someone overcome personal problems, or to attain personal growth. In modern practice, it has evolved ino what is known as psychodynamic therapy, which will be discussed later. Biomedical therapy involves medication and/or medical procedures to treat psychological disorders. First, we will explore the various psychotherapeutic orientations outlined in the Table 16.1 below (many of these orientations were discussed in the Introduction chapter).
Table 16.1 Various Psychotherapy Techniques
Type
Description
Example
Psychodynamic psychotherapy
Talk therapy based on belief that the unconscious and childhood conflicts impact behavior
Patient talks about his past
Play therapy
Psychoanalytical therapy wherein interaction with toys is used instead of talk; used in child therapy
Patient (child) acts out family scenes with dolls
Behavior therapy
Principles of learning applied to change undesirable behaviors
Patient learns to overcome fear of elevators through several stages of relaxation techniques
Cognitive therapy
Awareness of cognitive process helps patients eliminate thought patterns that lead to distress
Patient learns not to overgeneralize failure based on single failure
Cognitive-behavioral therapy
Work to change cognitive distortions and self-defeating behaviors
Patient learns to identify self-defeating behaviors to overcome an eating disorder
Humanistic therapy
Increase self-awareness and acceptance through focus on conscious thoughts
Patient learns to articulate thoughts that keep her from achieving her goals
Psychotherapy Techniques: Psychoanalysis
Psychoanalysis was developed by Sigmund Freud and was the first form of psychotherapy. It was the dominant therapeutic technique in the early \(20^{th}\) century, but it has since waned significantly in popularity. Freud believed most of our psychological problems are the result of repressed impulses and trauma experienced in childhood, and he believed psychoanalysis would help uncover long-buried feelings. In a psychoanalyst’s office, you might see a patient lying on a couch speaking of dreams or childhood memories, and the therapist using various Freudian methods such as free association and dream analysis (See figure 16.9. In free association, the patient relaxes and then says whatever comes to mind at the moment. However, Freud felt that the ego would at times try to block, or repress, unacceptable urges or painful conflicts during free association. Consequently, a patient would demonstrate resistance to recalling these thoughts or situations. In dream analysis, a therapist interprets the underlying meaning of dreams.
Psychoanalysis is a therapy approach that typically takes years. Over the course of time, the patient reveals a great deal about himself to the therapist. Freud suggested that during this patient-therapist relationship, the patient comes to develop strong feelings for the therapist—maybe positive feelings, maybe negative feelings. Freud called this transference: the patient transfers all the positive or negative emotions associated with the patient’s other relationships to the psychoanalyst. For example, Crystal is seeing a psychoanalyst. During the years of therapy, she comes to see her therapist as a father figure. She transfers her feelings about her father onto her therapist, perhaps in an effort to gain the love and attention she did not receive from her own father.
Figure 16.9 This is the famous couch in Freud’s consulting room. Patients were instructed to lie comfortably on the couch and to face away from Freud in order to feel less inhibited and to help them focus. Today, a psychotherapy patient is not likely to lie on a couch; instead he is more likely to sit facing the therapist (Prochaska & Norcross, 2010). (credit: Robert Huffstutter)
Today, Freud’s psychoanalytical perspective has been expanded upon by the developments of subsequent theories and methodologies: the psychodynamic perspective. This approach to therapy remains centered on the role of people’s internal drives and forces, but treatment is less intensive than Freud’s original model.
Play therapy is often used with children since they are not likely to sit on a couch and recall their dreams or engage in traditional talk therapy. This technique uses a therapeutic process of play to “help clients prevent or resolve psychosocial difficulties and achieve optimal growth” (O’Connor, 2000, p. 7). The idea is that children play out their hopes, fantasies, and traumas while using dolls, stuffed animals, and sandbox figurines (See figure 16.10). Play therapy can also be used to help a therapist make a diagnosis. The therapist observes how the child interacts with toys (e.g., dolls, animals, and home settings) in an effort to understand the roots of the child’s disturbed behavior. Play therapy can be nondirective or directive. In nondirective play therapy, children are encouraged to work through their problems by playing freely while the therapist observes (LeBlanc & Ritchie, 2001). In directive play therapy, the therapist provides more structure and guidance in the play session by suggesting topics, asking questions, and even playing with the child (Harter, 1977).
Figure 15.10 This type of play therapy is known as sandplay or sandtray therapy. Children can set up a three-dimensional world using various figures and objects that correspond to their inner state (Kalff, 1991). (credit: Kristina Walter)
Psychotherapy: Behavior Therapy
In psychoanalysis, therapists help their patients look into their past to uncover repressed feelings. In behavior therapy, a therapist employs principles of learning to help clients change undesirable behaviors—rather than digging deeply into one’s unconscious. Therapists with this orientation believe that dysfunctional behaviors, like phobias and bedwetting, can be changed by teaching clients new, more constructive behaviors. Behavior therapy employs both classical and operant conditioning techniques to change behavior.
One type of behavior therapy utilizes classical conditioning techniques. Therapists using these techniques believe that dysfunctional behaviors are conditioned responses. Applying the conditioning principles developed by Ivan Pavlov, these therapists seek to recondition their clients and thus change their behavior. Emmie is eight years old, and frequently wets her bed at night. She’s been invited to several sleepovers, but she won’t go because of her problem. Using a type of conditioning therapy, Emmie begins to sleep on a liquid-sensitive bed pad that is hooked to an alarm. When moisture touches the pad, it sets off the alarm, waking up Emmie. When this process is repeated enough times, Emmie develops an association between urinary relaxation and waking up, and this stops the bedwetting. Emmie has now gone three weeks without wetting her bed and is looking forward to her first sleepover this weekend.
One commonly used classical conditioning therapeutic technique is counterconditioning: a client learns a new response to a stimulus that has previously elicited an undesirable behavior. Two counterconditioning techniques are aversive conditioning and exposure therapy. Aversive conditioning uses an unpleasant stimulus to stop an undesirable behavior. Therapists apply this technique to eliminate addictive behaviors, such as smoking, nail biting, and drinking. In aversion therapy, clients will typically engage in a specific behavior (such as nail biting) and at the same time are exposed to something unpleasant, such as a mild electric shock or a bad taste. After repeated associations between the unpleasant stimulus and the behavior, the client can learn to stop the unwanted behavior.
Aversion therapy has been used effectively for years in the treatment of alcoholism (Davidson, 1974; Elkins, 1991; Streeton & Whelan, 2001). One common way this occurs is through a chemically based substance known as Antabuse. When a person takes Antabuse and then consumes alcohol, uncomfortable side effects result including nausea, vomiting, increased heart rate, heart palpitations, severe headache, and shortness of breath. Antabuse is repeatedly paired with alcohol until the client associates alcohol with unpleasant feelings, which decreases the client’s desire to consume alcohol. Antabuse creates a conditioned aversion to alcohol because it replaces the original pleasure response with an unpleasant one.
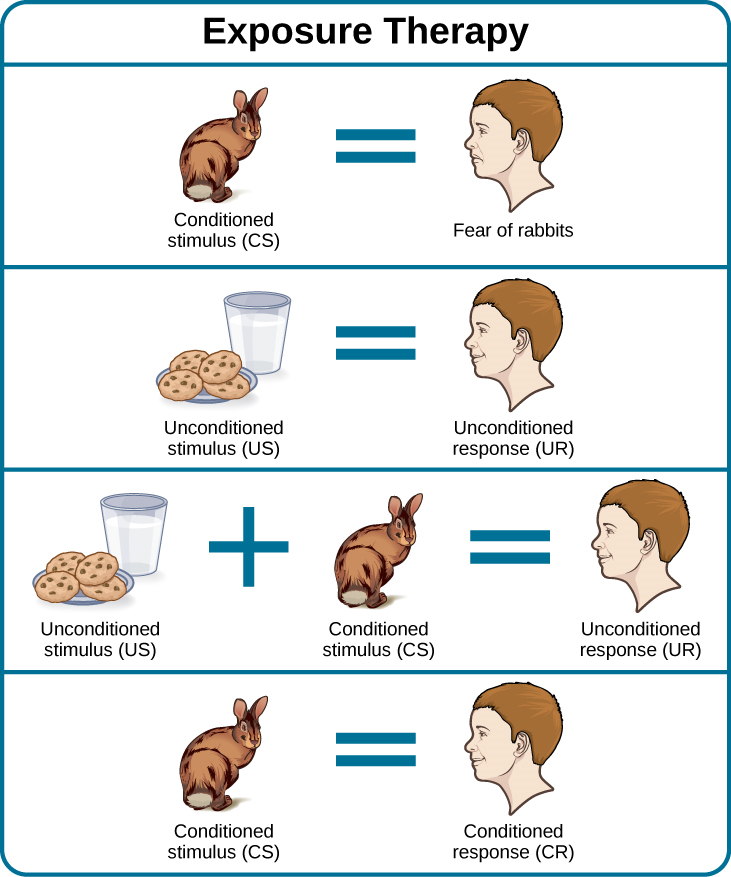
In exposure therapy, a therapist seeks to treat clients’ fears or anxiety by presenting them with the object or situation that causes their problem, with the idea that they will eventually get used to it. This can be done via reality, imagination, or virtual reality. Exposure therapy was first reported in 1924 by Mary Cover Jones, who is considered the mother of behavior therapy. Jones worked with a boy named Peter who was afraid of rabbits. Her goal was to replace Peter’s fear of rabbits with a conditioned response of relaxation, which is a response that is incompatible with fear (See figure 16.11). How did she do it? Jones began by placing a caged rabbit on the other side of a room with Peter while he ate his afternoon snack. Over the course of several days, Jones moved the rabbit closer and closer to where Peter was seated with his snack. After two months of being exposed to the rabbit while relaxing with his snack, Peter was able to hold the rabbit and pet it while eating (Jones, 1924).
Figure 16.11 Exposure therapy seeks to change the response to a conditioned stimulus (CS). An unconditioned stimulus is presented over and over just after the presentation of the conditioned stimulus. This figure shows conditioning as conducted in Mary Cover Jones’ 1924 study.
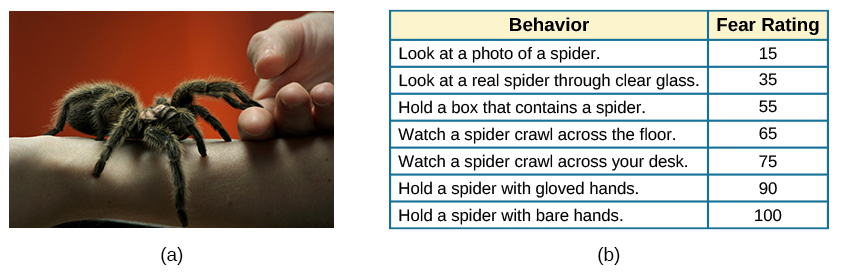
Thirty years later, Joseph Wolpe (1958) refined Jones’s techniques, giving us the behavior therapy technique of exposure therapy that is used today. A popular form of exposure therapy is systematic desensitization, wherein a calm and pleasant state is gradually associated with increasing levels of anxiety-inducing stimuli. The idea is that you can’t be nervous and relaxed at the same time. Therefore, if you can learn to relax when you are facing environmental stimuli that make you nervous or fearful, you can eventually eliminate your unwanted fear response (Wolpe, 1958) (See figure 16.12 below).
Figure 16.12 This person suffers from arachnophobia (fear of spiders). Through exposure therapy he is learning how to face his fear in a controlled, therapeutic setting. (credit: “GollyGforce – Living My Worst Nightmare”/Flickr)
For example, Jayden is terrified of elevators. Nothing bad has ever happened to him on an elevator, but he’s so afraid of elevators that he will always take the stairs. That wasn’t a problem when Jayden worked on the second floor of an office building, but now he has a new job—on the 29th floor of a skyscraper in downtown Los Angeles. Jayden knows he can’t climb 29 flights of stairs in order to get to work each day, so he decided to see a behavior therapist for help. The therapist asks Jayden to first construct a hierarchy of elevator-related situations that elicit fear and anxiety. They range from situations of mild anxiety such as being nervous around the other people in the elevator, to the fear of getting an arm caught in the door, to panic-provoking situations such as getting trapped or the cable snapping. Next, the therapist uses progressive relaxation. They teach Jayden how to relax each of his muscle groups so that he achieves a drowsy, relaxed, and comfortable state of mind. Once he’s in this state, the therapist asks Jayden to imagine a mildly anxiety-provoking situation. Jayden is standing in front of the elevator thinking about pressing the call button.
If this scenario causes Jayden anxiety, he lifts his finger. The therapist would then tell Jayden to forget the scene and return to his relaxed state. They repeat this scenario over and over until Jayden can imagine himself pressing the call button without anxiety. Over time the therapist and Jayden use progressive relaxation and imagination to proceed through all of the situations on Jayden’s hierarchy until he becomes desensitized to each one. After this, Jayden and the therapist begin to practice what he only previously envisioned in therapy, gradually going from pressing the button to actually riding an elevator. The goal is that Jayden will soon be able to take the elevator all the way up to the 29th floor of his office without feeling any anxiety.
Sometimes, it’s too impractical, expensive, or embarrassing to re-create anxiety- producing situations, so a therapist might employ virtual reality exposure therapy by using a simulation to help conquer fears. Virtual reality exposure therapy has been used effectively to treat numerous anxiety disorders such as the fear of public speaking, claustrophobia (fear of enclosed spaces), aviophobia (fear of flying), and post-traumatic stress disorder (PTSD), a trauma and stressor-related disorder (Gerardi, Cukor, Difede, Rizzo, & Rothbaum, 2010).
Link to Learning
A new virtual reality exposure therapy is being used to treat PTSD in soldiers. Virtual Iraq is a simulation that mimics Middle Eastern cities and desert roads with situations similar to those soldiers experienced while deployed in Iraq. This method of virtual reality exposure therapy has been effective in treating PTSD for combat veterans. Approximately 80% of participants who completed treatment saw clinically significant reduction in their symptoms of PTSD, anxiety, and depression (Rizzo et al., 2010). Watch this Virtual Iraq video that shows soldiers being treated via simulation to learn more.
Some behavior therapies employ operant conditioning. Recall what you learned about operant conditioning: We have a tendency to repeat behaviors that are reinforced. What happens to behaviors that are not reinforced? They become extinguished. These principles can be applied to help people with a wide range of psychological problems. For instance, operant conditioning techniques designed to reinforce positive behaviors and punish unwanted behaviors have been an effective tool to help children with autism (Lovaas, 1987, 2003; Sallows & Graupner, 2005; Wolf & Risley, 1967). This technique is called Applied Behavior Analysis (ABA). In this treatment, child-specific reinforcers (e.g., stickers, praise, candy, bubbles, and extra play time) are used to reward and motivate autistic children when they demonstrate desired behaviors such as sitting on a chair when requested, verbalizing a greeting, or making eye contact. Punishment such as a timeout or a sharp “No!” from the therapist or parent might be used to discourage undesirable behaviors such as pinching, scratching, and pulling hair.
One popular operant conditioning intervention is called the token economy. This involves a controlled setting where individuals are reinforced for desirable behaviors with tokens, such as a poker chip, that can be exchanged for items or privileges. Token economies are often used in psychiatric hospitals to increase patient cooperation and activity levels. Patients are rewarded with tokens when they engage in positive behaviors (e.g., making their beds, brushing their teeth, coming to the cafeteria on time, and socializing with other patients). They can later exchange the tokens for extra TV time, private rooms, visits to the canteen, and so on (Dickerson, Tenhula, & Green-Paden, 2005).
Psychotherapy: Cognitive Therapy
Cognitive therapy is a form of psychotherapy that focuses on how a person’s thoughts lead to feelings of distress. The idea behind cognitive therapy is that how you think determines how you feel and act. Cognitive therapists help their clients change dysfunctional thoughts in order to relieve distress. They help a client see how they misinterpret a situation (cognitive distortion). For example, a client may overgeneralize. Because Ray failed one test in his Psychology 101 course, he feels he is stupid and worthless. These thoughts then cause his mood to worsen. Therapists also help clients recognize when they blow things out of proportion. Because Ray failed his Psychology 101 test, he has concluded that he’s going to fail the entire course and probably flunk out of college altogether. These errors in thinking have contributed to Ray’s feelings of distress. His therapist will help him challenge these irrational beliefs, focus on their illogical basis, and correct them with more logical and rational thoughts and beliefs.
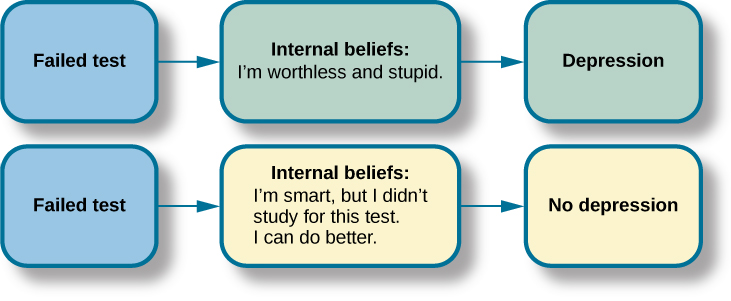
Cognitive therapy was developed by psychiatrist Aaron Beck in the 1960s. His initial focus was on depression and how a client’s self-defeating attitude served to maintain a depression despite positive factors in her life (Beck, Rush, Shaw, & Emery, 1979) (See figure 16.3). Through questioning, a cognitive therapist can help a client recognize dysfunctional ideas, challenge catastrophizing thoughts about themselves and their situations, and find a more positive way to view things (Beck, 2011).
Figure 16.3 Your emotional reactions are the result of your thoughts about the situation rather than the situation itself. For instance, if you consistently interpret events and emotions around the themes of loss and defeat, then you are likely to be depressed. Through therapy, you can learn more logical ways to interpret situations.
Psychotherapy: Cognitive-Behavioral Therapy
Cognitive-behavioral therapists focus much more on present issues than on a patient’s childhood or past, as in other forms of psychotherapy. One of the first forms of cognitive-behavioral therapy was rational emotive therapy (RET), which was founded by Albert Ellis and grew out of his dislike of Freudian psychoanalysis (Daniel, n.d.). Behaviorists such as Joseph Wolpe also influenced Ellis’s therapeutic approach (National Association of Cognitive-Behavioral Therapists, 2009).
Cognitive-behavioral therapy (CBT) helps clients examine how their thoughts affect their behavior. It aims to change cognitive distortions and self-defeating behaviors. In essence, this approach is designed to change the way people think as well as how they act. It is similar to cognitive therapy in that CBT attempts to make individuals aware of their irrational and negative thoughts and helps people replace them with new, more positive ways of thinking. It is also similar to behavior therapies in that CBT teaches people how to practice and engage in more positive and healthy approaches to daily situations. In total, hundreds of studies have shown the effectiveness of cognitive-behavioral therapy in the treatment of numerous psychological disorders such as depression, PTSD, anxiety disorders, eating disorders, bipolar disorder, and substance abuse (Beck Institute for Cognitive Behavior Therapy, n.d.). For example, CBT has been found to be effective in decreasing levels of hopelessness and suicidal thoughts in previously suicidal teenagers (Alavi, Sharifi, Ghanizadeh, & Dehbozorgi, 2013). Cognitive-behavioral therapy has also been effective in reducing PTSD in specific populations, such as transit workers (Lowinger & Rombom, 2012).
Cognitive-behavioral therapy aims to change cognitive distortions and self-defeating behaviors using techniques like the ABC model. With this model, there is an Action (sometimes called an activating event), the Belief about the event, and the Consequences of this belief. Let’s say, Jon and Joe both go to a party. Jon and Joe each have met a young woman at the party: Jon is talking with Megan most of the party, and Joe is talking with Amanda. At the end of the party, Jon asks Megan for her phone number and Joe asks Amanda. Megan tells Jon she would rather not give him her number, and Amanda tells Joe the same thing. Both Jon and Joe are surprised, as they thought things were going well. What can Jon and Joe tell themselves about why the women were not interested? Let’s say Jon tells himself he is a loser, or is ugly, or “has no game.” Jon then gets depressed and decides not to go to another party, which starts a cycle that keeps him depressed. Joe tells himself that he had bad breath, goes out and buys a new toothbrush, goes to another party, and meets someone new.
Jon’s belief about what happened results in a consequence of further depression, whereas Joe’s belief does not. Jon is internalizing the attribution or reason for the rebuffs, which triggers his depression. On the other hand, Joe is externalizing the cause, so his thinking does not contribute to feelings of depression. Cognitive-behavioral therapy examines specific maladaptive and automatic thoughts and cognitive distortions. Some examples of cognitive distortions are all-or-nothing thinking, overgeneralization, and jumping to conclusions. In overgeneralization, someone takes a small situation and makes it huge—for example, instead of saying, “This particular woman was not interested in me,” the man says, “I am ugly, a loser, and no one is ever going to be interested in me.”
All or nothing thinking, which is a common type of cognitive distortion for people suffering from depression, reflects extremes. In other words, everything is black or white. After being turned down for a date, Jon begins to think, “No woman will ever go out with me. I’m going to be alone forever.” He begins to feel anxious and sad as he contemplates his future.
The third kind of distortion involves jumping to conclusions—assuming that people are thinking negatively about you or reacting negatively to you, even though there is no evidence. Consider the example of Savannah and Hillaire, who recently met at a party. They have a lot in common, and Savannah thinks they could become friends. She calls Hillaire to invite her for coffee. Since Hillaire doesn’t answer, Savannah leaves her a message. Several days go by and Savannah never hears back from her potential new friend. Maybe Hillaire never received the message because she lost her phone or she is too busy to return the phone call. But if Savannah believes that Hillaire didn’t like Savannah or didn’t want to be her friend, she is demonstrating the cognitive distortion of jumping to conclusions.
How effective is CBT? One client said this about his cognitive-behavioral therapy:
"I have had many painful episodes of depression in my life, and this has had a negative effect on my career and has put considerable strain on my friends and family. The treatments I have received, such as taking antidepressants and psychodynamic counseling, have helped [me] to cope with the symptoms and to get some insights into the roots of my problems. CBT has been by far the most useful approach I have found in tackling these mood problems. It has raised my awareness of how my thoughts impact on my moods. How the way I think about myself, about others and about the world can lead me into depression. It is a practical approach, which does not dwell so much on childhood experiences, whilst acknowledging that it was then that these patterns were learned. It looks at what is happening now, and gives tools to manage these moods on a daily basis." (Martin, 2007, n.p.)
Psychotherapy: Humanistic Therapy
Humanistic psychology focuses on helping people achieve their potential. So it makes sense that the goal of humanistic therapy is to help people become more self-aware and accepting of themselves. In contrast to psychoanalysis, humanistic therapists focus on conscious rather than unconscious thoughts. They also emphasize the patient’s present and future, as opposed to exploring the patient’s past.
Psychologist Carl Rogers developed a therapeutic orientation known as Rogerian, or client-centered therapy. Note the change from patients to clients. Rogers (1951) felt that the term patient suggested the person seeking help was sick and looking for a cure. Since this is a form of nondirective therapy, a therapeutic approach in which the therapist does not give advice or provide interpretations but helps the person to identify conflicts and understand feelings, Rogers (1951) emphasized the importance of the person taking control of his own life to overcome life’s challenges.
In client-centered therapy, the therapist uses the technique of active listening. In active listening, the therapist acknowledges, restates, and clarifies what the client expresses. Therapists also practice what Rogers called unconditional positive regard, which involves not judging clients and simply accepting them for who they are. Rogers (1951) also felt that therapists should demonstrate genuineness, empathy, and acceptance toward their clients because this helps people become more accepting of themselves, which results in personal growth.
Evaluating Various Forms of Psychotherapy
How can we assess the effectiveness of psychotherapy? Is one technique more effective than another? For anyone considering therapy, these are important questions. According to the American Psychological Association, three factors work together to produce successful treatment. The first is the use of evidence-based treatment that is deemed appropriate for your particular issue. The second important factor is the clinical expertise of the psychologist or therapist. The third factor is your own characteristics, values, preferences, and culture. Many people begin psychotherapy feeling like their problem will never be resolved; however, psychotherapy helps people see that they can do things to make their situation better. Psychotherapy can help reduce a person’s anxiety, depression, and maladaptive behaviors. Through psychotherapy, individuals can learn to engage in healthy behaviors designed to help them better express emotions, improve relationships, think more positively, and perform more effectively at work or school.
Many studies have explored the effectiveness of psychotherapy. For example, one large-scale study that examined \(16\) meta-analyses of CBT reported that it was equally effective or more effective than other therapies in treating PTSD, generalized anxiety disorder, depression, and social phobia (Butlera, Chapmanb, Formanc, & Becka, 2006). Another study found that CBT was as effective at treating depression (\(43\%\) success rate) as prescription medication (\(50\%\) success rate) compared to the placebo rate of \(25\%\) (DeRubeis et al., 2005). Another meta-analysis found that psychodynamic therapy was also as effective at treating these types of psychological issues as CBT (Shedler, 2010). However, no studies have found one psychotherapeutic approach more effective than another (Abbass, Kisely, & Kroenke, 2006; Chorpita et al., 2011), nor have they shown any relationship between a client’s treatment outcome and the level of the clinician’s training or experience (Wampold, 2007). Regardless of which type of psychotherapy an individual chooses, one critical factor that determines the success of treatment is the person’s relationship with the psychologist or therapist.
Biomedical Therapies
Individuals can be prescribed biologically based treatments or psychotropic medications that are used to treat mental disorders. While these are often used in combination with psychotherapy, they also are taken by individuals not in therapy. This is known as biomedical therapy. Medications used to treat psychological disorders are called psychotropic medications and are prescribed by medical doctors, including psychiatrists. In Louisiana and New Mexico, psychologists are able to prescribe some types of these medications (American Psychological Association, 2014).
Different types and classes of medications are prescribed for different disorders. An individual with depression might be given an antidepressant, an individual with bipolar disorder might be given a mood stabilizer, and an individual with schizophrenia might be given an antipsychotic. These medications treat the symptoms of a psychological disorder by altering the levels or effects of neurotransmitters. For example, each type of antidepressant affects a different neurotransmitter, such as SSRI (selective serotonin reuptake inhibitor) antidepressants that increase the level of the neurotransmitter serotonin, and SNRI (serotonin-norepinephrine reuptake inhibitor) antidepressants that increase the levels of both serotonin and norepinephrine. They can help people feel better so that they can function on a daily basis, but they do not cure the disorder. Some people may only need to take a psychotropic medication for a short period of time. Others with severe disorders like bipolar disorder or schizophrenia may need to take psychotropic medication for a long time.
Psychotropic medications are a popular treatment option for many types of disorders, and research suggests that they are most effective when combined with psychotherapy. This is especially true for the most common mental disorders, such as depressive and anxiety disorders (Cuijpers et al, 2014). When considering adding medication as a treatment option, individuals should know that some psychotropic medications have very concerning side effects. Table 16.2 shows the commonly prescribed types of medications, how they are used, and some of the potential side effects that may occur.
Schizophrenia and other types of severe thought disorders
Haldol, Mellaril, Prolixin, Thorazine
Treat positive psychotic symptoms such as auditory and visual hallucinations, delusions, and paranoia by blocking the neurotransmitter dopamine
Long-term use can lead to tardive dyskinesia, involuntary movements of the arms, legs, tongue and facial muscles, resulting in Parkinson’s-like tremors
Atypical Antipsychotics (developed in the late 1980s)
Schizophrenia and other types of severe thought disorders
Abilify, Risperdal, Clozaril
Treat the negative symptoms of schizophrenia, such as withdrawal and apathy, by targeting both dopamine and serotonin receptors; newer medications may treat both positive and negative symptoms
Can increase the risk of obesity and diabetes as well as elevate cholesterol levels; constipation, dry mouth, blurred vision, drowsiness, and dizziness
Another biologically based treatment that continues to be used, although infrequently, is electroconvulsive therapy (ECT) (formerly known by its unscientific name as electroshock therapy). It involves using an electrical current to induce seizures to help alleviate the effects of severe depression. The exact mechanism is unknown, although it does help alleviate symptoms for people with severe depression who have not responded to traditional drug therapy (Pagnin, de Queiroz, Pini, & Cassano, 2004). About \(85\%\) of people treated with ECT improve (Reti, n.d.). However, the memory loss associated with repeated administrations has led to it being implemented as a last resort (Donahue, 2000; Prudic, Peyser, & Sackeim, 2000). A more recent alternative is transcranial magnetic stimulation (TMS), a procedure approved by the FDA in 2008 that uses magnetic fields to stimulate nerve cells in the brain to improve depression symptoms; it is used when other treatments have not worked (Mayo Clinic, 2012).
DIG DEEPER: Evidence-based Practice
A buzzword in therapy today is evidence-based practice. However, it’s not a novel concept but one that has been used in medicine for at least two decades. Evidence-based practice is used to reduce errors in treatment selection by making clinical decisions based on research (Sackett & Rosenberg, 1995). In any case, evidence-based treatment is on the rise in the field of psychology. So what is it, and why does it matter? In an effort to determine which treatment methodologies are evidenced-based, professional organizations such as the American Psychological Association (APA) have recommended that specific psychological treatments be used to treat certain psychological disorders (Chambless & Ollendick, 2001). According to the APA (2005), “Evidence-based practice in psychology (EBPP) is the integration of the best available research with clinical expertise in the context of patient characteristics, culture, and preferences” (p. 1).
The foundational idea behind evidence based treatment is that best practices are determined by research evidence that has been compiled by comparing various forms of treatment (Charman & Barkham, 2005). These treatments are then operationalized and placed in treatment manuals—trained therapists follow these manuals. The benefits are that evidence-based treatment can reduce variability between therapists to ensure that a specific approach is delivered with integrity (Charman & Barkham, 2005). Therefore, clients have a higher chance of receiving therapeutic interventions that are effective at treating their specific disorder. While EBPP is based on randomized control trials, critics of EBPP reject it stating that the results of trials cannot be applied to individuals and instead determinations regarding treatment should be based on a therapist’s judgment (Mullen & Streiner, 2004).