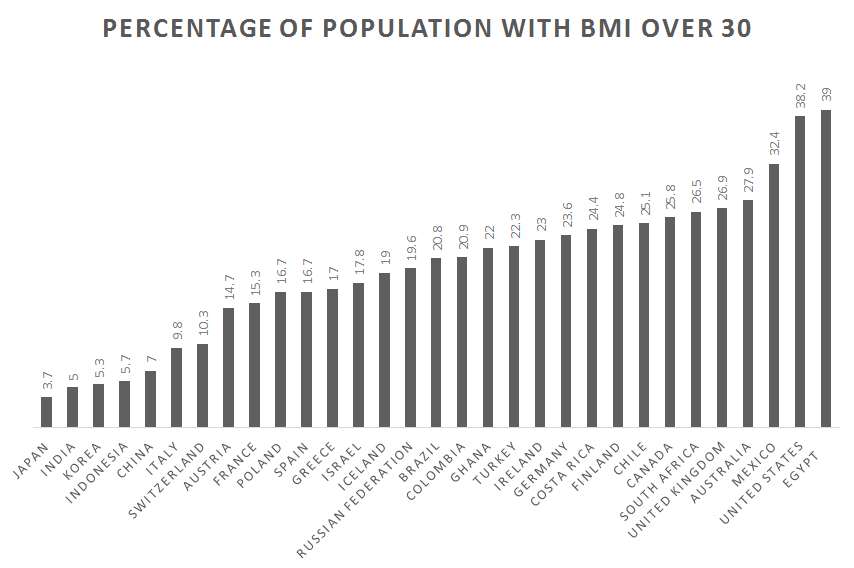
According to the World Health Organization (2017), 1.9 billion of the world’s people are overweight and 650 million of these are obese. In the United States, 70% of Americans are overweight, and 40% of these meet the criteria for obesity. For the first time in human history, most of the world’s population lives in countries where overweight and obesity kill more people than hunger (Figure 16.4). Improvements in public health and food production have allowed a greater number of people to live past childhood and to have enough to eat. This does not include everyone. Many people still struggle with poverty, hunger, and disease, even in the wealthiest of nations, including the United States. On a global scale, however, many people not only have enough food to survive but also to gain weight—enough extra weight to cause health problems.
Although studies show differences in daily energy expenditure between foraging and farming populations compared with industrialized peoples, the major contributor to obesity in Western populations is energy intake (Pontzer et al. 2012). Many people not only eat too much but too much of the wrong things. Biological anthropologist Leslie Lieberman (2006) argues that contemporary humans continue to rely on cues from foraging strategies of our evolutionary past that are now counterproductive in the obesogenic environments in which we now live.
Examine your own eating habits in the context of how humans once hunted and gathered. Humans once relied on visual cues to find food, often traveled long distances to obtain it, then transported it back to our home base. There they may have had to process it by hand to render it edible. Think of how much less energy it takes to find food now. If we have the financial resources, we can acquire big energy payoffs by simply sitting at home and using an app on our mobile phone to place an order for delivery. And, voila! High-calorie (if not highly nutritious) food arrives at our door. Should we venture out for food, search time is reduced by signage and advertising directing us toward high-density “patches” where food is available 24 hours a day. These include vending machines, gas stations, and fast-food outlets. Travel time is minimal and little human energy is used in the process (Lieberman 2006).
Foods are also prepackaged and prepared in ways that allow us to eat large quantities quickly. Think French fries or chicken nuggets, which we can easily eat with our hands while doing other things, like driving or watching television, rendering eating mindless and allowing us to take in food faster than our endocrine systems can tell us we are getting full. Modern “patches” offer low-fiber, calorie-dense resources, which allow us to eat larger quantities, a problem already encouraged by larger portion sizes (Lieberman 2006). Processed foods are also engineered to appeal to human preferences for sweet tastes and fatty, creamy textures (Moss 2013). Remember from earlier chapters that natural selection favored depth perception, color vision, grasping hands, and coordinated eye-hand movements as general primate traits. Advertising and packaging now use our color vision against us, attracting us to products that have little nutritional value but that play to our evolutionary predisposition toward variety. Remember those 50 different nutrients we require? That variety is now presented to us in the form of 55 different flavors of Oreo cookies (Cerón 2017), which we take out of the package and dip in milk using our hand-eye coordination and depth perception.
Even if we are ostensibly eating the same things our ancestors did, these foods are nothing alike. Take potatoes, for example. One medium-sized, plain, baked potato is a healthy food, especially if we eat the skin too. It contains 110 calories, 0 grams of fat, 26 grams of carbohydrates, and 3 grams of protein, plus 30% of the U.S. Recommended Daily Allowance (RDA) of vitamin C, 10% of vitamin B6, 15% of potassium, and no sodium (Potato USA). In contrast, a medium order of McDonald’s fries, which takes the potato and adds salt and fat, contains 340 calories, 16 grams of fat, 44 grams of carbohydrates, 4 grams of protein, and 230 mg of sodium (McDonalds). Potato chips take food processing to a whole new level, removing even more nutrition and adding a host of additional ingredients, including oils, preservatives, and artificial flavorings and colors (Moss 2013). Take Ruffles Loaded Bacon and Cheddar Potato Skins Potato Chips as an example (St. Pierre 2018). The number of ingredients increases from one to 11 to 35 as we move from the potato to the potato chip, moving further from nature with each step (Figure 16.5). It should be noted that the nutritional information for the potato chips is based on a serving size of 11 chips, an amount likely smaller than many people eat. Many sweet, fatty, salty foods like fries and chips are cheap, which is why many people choose to eat them (Moss 2013). The price of a medium-sized order of McDonald’s fries as of this writing is US$1.79, and the potato chips are $2.98 for an 8.5-ounce bag. A single potato prewrapped for microwaving is available in many supermarkets for US$1.99 but requires access to a microwave and eating utensils, making it less convenient.
Potatoes, vegetable oil (sunflower, corn, and/or canola oil), bacon and chedder loaded potato skins seasoning (maltodextrin – made from corn) salt, cheddar cheese (milk, cheese cultures, salt enzymes), sour cream (cultured cream, skin milk), whey, dried onion, monosodium.
Not only have we transformed the food supply and our eating in ways that are detrimental to our health, but these changes have been accompanied by reductions in physical activity. Sedentarism is built into contemporary lifestyles. Think of how much time you spent sitting down today. Some of it may have been in class or at work, some may have been driving a car or perhaps binge-watching your favorite show, playing a video game, or checking in on social media. An inactive lifestyle is almost dictated by the digital age (Lucock et al. 2014). Levels of physical activity in many countries are now so low that large portions of the population are completely sedentary, including one in five Americans (CDC 2022). For a species whose biology evolved in an environment where walking, lifting, and carrying were part of daily life, this is unhealthy and often leads to weight gain.
Biology and Genetics of Weight
Research indicates multiple genetic variants influence weight gain, and they are not spread evenly among human populations. Tuomo Rankinen and colleagues (2006) identified 127 genes associated with obesity, of which 22 contributed to weight gain. Claude Bouchard (2007) then identified five categories of obesity-promoting genotypes. These genotypes promote sedentarism, result in low metabolism, and lead to poor regulation of appetite, and a propensity to overeat. An example of the impact such genotypes can have in an environment of plenty is found among the population of the Micronesian island of Nauru. Historically, the island was geographically isolated and the food supply was unpredictable. These conditions favored genotypes that promoted the ability to rapidly build up and store fat in times of food availability. In Nauruans, there are two genetic variants favoring weight gain and insulin resistance, and both are associated with obesity and type 2 diabetes. One variant is also associated with hypertension. One of these variants is also found in Pima Indians, who live in parts of Arizona and Mexico. In the Pima, this variant is associated with a high body mass index (BMI) and type 2 diabetes, although it is not associated with the same outcomes in Japanese and British subjects (de Silva et al. 1999). The other variant was analyzed in Finnish and South Indian populations, neither of whom experienced the same outcome as Nauruans. This suggests these alleles may act as modifying genes for type 2 diabetes in some population groups (Baker et al. 1994). Unfortunately, Nauruans are one of those groups. Eventually, they became wealthy through phosphate mining on the island, gaining access to a calorie-rich Western diet of imported foods and developing a sedentary lifestyle. This resulted in rates of type 2 diabetes as high as 30–40% in Nauruans over the age of 15, which became the leading cause of death (Lucock et al. 2014), something Nauruans are taking seriously (Figure 16.6).
Factors other than biology influence which populations that carry a genetic predisposition to diabetes actually express it. The Pima Indians of Arizona, for example, were seriously impacted by U.S. government policies that affected water rights, forcing the population away from subsistence farming to dependence on government handouts and convenience food. This resulted in a significant loss of physical activity, malnutrition, and obesity. The Pima continue to experience hardship due to high rates of unemployment, poverty, and depression, sometimes made worse by alcoholism. In the absence of these pressures, the Pima were diabetes free for centuries prior, even though they relied on agriculture for subsistence, suggesting genetics alone is not responsible for high rates of obesity and diabetes in current Pima Indian populations (Smith-Morris 2004).
Figure 16.7: Medical complications of obesity include stroke, sleep apnea, lung disease, liver disease, gallstones, cancer, heart disease, diabetes, pancreatitis, abnormal periods and infertility, arthritis, inflamed veins, and gout. Credit: Medical complications of obesity by the Centers for Disease Control and Prevention (CDC) has been modified (color changed and cancer list shortened) and is in the public domain.
Obesity also has an epigenetic component. You learned about epigenetics in Chapter 3. With regard to obesity, epigenetics is counterintuitive in that mothers who do not take in enough calories during pregnancy often give birth to babies who grow up to be fat. What takes place is the fetus receives signals during pregnancy from its mother through the placenta and intrauterine environment about environmental conditions outside of the womb, in this case food insecurity. These signals encourage the turning on and off of genes related to metabolism. This alters the phenotype of the fetus so that if the child is born into an environment where food is plentiful, it will put on weight rapidly whenever possible, leading to obesity and related diseases later in life. If the child is a girl, her own eggs are formed in utero with the same genetic changes coded in, meaning she will pass along this same genetic predisposition to gain weight to her children. Hence, a biological propensity toward obesity can continue across generations (Worthman and Kuzara 2005). Epigenetic changes to genes that promote weight gain are argued to be partly responsible for the rapid rise in obesity and diabetes in developing countries gaining access to Western diets (Stearns, Nesse, and Haig 2008).
Obesity and overweight put a strain on several biological systems of the body, including the circulatory, endocrine, and skeletal systems, contributing to hypertension, heart disease, stroke, diabetes, and osteoarthritis (Figure 16.7). Obesity also elevates the risk of cancers of the breast, endometrium, kidney, colon, esophagus, stomach, pancreas, and gallbladder (National Institutes of Health 2017; Vucenik and Stains 2012). Diabetes—one of the fastest-growing health conditions around the globe (WHO 2016) and one tightly connected to obesity and overweight—is the focus of the following Special Topics box.
Special Topic: Diabetes
Diabetes mellitus is an endocrine disorder characterized by excessively high blood glucose levels (Martini et al. 2013). According to a report released by the World Health Organization, the number of people living with diabetes is growing in all regions of the world. Rates of diabetes have nearly doubled in the past three decades, largely due to increases in obesity and sugary diets (WHO 2016). One in 10 people around the world, 537 million people, now have diabetes, and three out of four live in low- and middle-income countries (IDF 2022). In the United States, 37 million people have diabetes (CDC 2020), where the disease is rising fastest among millennials (those ages 20–40) (BCBSA 2017), and one in every two adults with diabetes is undiagnosed (IDF 2022). Obesity and diabetes are linked: obesity causes a diet-related disease (diabetes) because of humans’ evolved metabolic homeostasis mechanism, which is poorly suited to contemporary energy environments (Lucock et al. 2014).
To function properly, cells need a steady fuel supply. Blood sugar (glucose) is the fuel for most cells in the body, and the body produces the hormone insulin to help move glucose into cells that need it (Figure 16.8). Foods that most readily supply glucose to your bloodstream are carbohydrates, especially starchy foods like potatoes or sweet, sugary foods like candy and soda. The body can also convert other types of foods, including protein-rich foods (e.g., lean meats) and fatty foods (e.g., vegetable oils and butter), into blood sugar in the liver via gluconeogenesis. Insulin’s main job is to tell your cells when to take up glucose. The cell also has to listen to the signal and mobilize the glucose transporters. This not only allows your cells to get the energy they need, but it also keeps blood sugar from building up to dangerously high levels when you are at rest.
Figure 16.8: Carbohydrates are eaten and broken down into simple sugars (e.g., glucose). Glucose enters the bloodstream from the intestines, and the increase in glucose stimulates the pancreas to release insulin into the bloodstream. Insulin deposits glucose in the muscles and fat cells, where it is stored and used for energy. Credit: Glucose metabolism (Figure 16.7) original to Explorations: An Open Invitation to Biological Anthropology by Mary Nelson is under a CC BY-NC 4.0 License.
This system has limits. Like the rest of our biology, it evolved during several million years when sugar was hard to come by and carbohydrates took the form of fresh foods with a low glycemic index (GI). Our ancestors were also active throughout the day, taking pressure off of the endocrine system. Now, sedentary lifestyles and processed-food diets cause many of us to take in more calories—and especially more carbohydrates—than our bodies can handle. There is only so much blood sugar your cells can absorb. Many modern populations are taxing those limits. After years of being asked by insulin to take in more glucose than they can use, cells eventually stop responding (McKee and McKee 2015). This is called type 2 diabetes or insulin resistance, which accounts for 90–95% of diabetes cases in the United States (Figure 16.9). type 1 diabetes is believed to be caused by an autoimmune response in which your immune system is attacking and destroying the insulin-producing cells in your pancreas (Figure 16.9). type 1 diabetes is a genetic condition that often shows up early in life, while type 2 is more lifestyle-related and develops over time.


 Baked Potato
Baked Potato Potato Chips
Potato Chips


