While a disorder such as obstructive sleep apnea—not breathing during the night—is very serious and has lethal consequences, it is also essential that other, seemingly more subtle sleep disorders, such as periodic limb movements, get diagnosed and treated. For example, if someone has daytime sleepiness, and sleep apnea has been ruled out, the person still needs to find out what is leading to their sleepiness. In chapter 1, we have covered sleep debt and its serious consequences, such as depression, stroke, heart attack, obesity, diabetes, and more. Therefore, we must not take lightly any condition that disrupts sleep. In my workshops, I have met people all over the world who tell me they had undergone sleep studies in which, after apnea was ruled out, they were sent on their way with no further investigation or advice. Or worse still, they were given a prescription for sleeping pills, which are not meant as a long-term solution and can lead to countless other problems with no benefit or, at most, perhaps twenty additional minutes of sleep a night. We need to advocate for ourselves and loved ones to get health-care practitioners to persevere until we know what is causing daytime drowsiness and get it treated. Our lives depend on it.
Insomnia
Many people who suffer from poor sleep think they have a disorder called insomnia. However, most people who believe this actually have a particular factor causing their poor sleep, and such factors can usually be addressed—the sleep is improved and insomnia goes away. It is rare for a person to have insomnia not caused by something else, such as stress, physical pain, medication, a psychiatric disorder, a physical illness, or poor sleep-health habits. These are what I mean by “factors” causing insomnia.
The most straightforward factors to address are poor sleep-health habits. Refer to chapter 1 to identify and determine strategies to attend to habits disturbing your sleep. That chapter also has detailed instructions for several techniques to alleviate insomnia as well as recommendations for effective treatments; the gold standard is cognitive behavioral therapy for insomnia. For many people, following the guidelines in chapter 1 will fix their sleep. If not, a sleep specialist can determine what other factors need to be addressed and develop a treatment approach. Once all these factors have been addressed, if the person is still not sleeping well, then a clinical sleep study may be necessary to identify an underlying sleep disorder causing the insomnia. But for most people, their sleep will be restored before they get to that stage.
Snoring
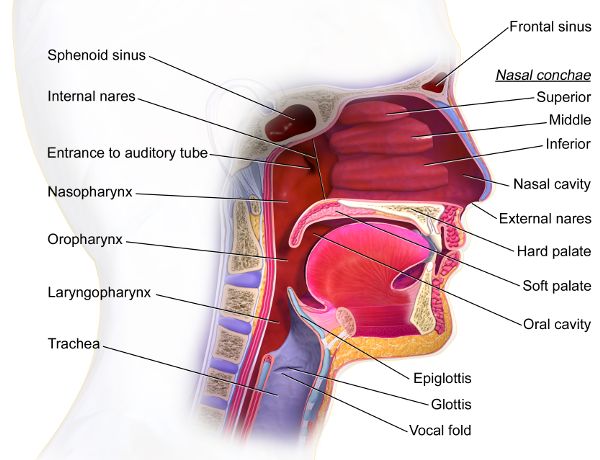
Have you ever noticed that if a snoring person rolls on their side, it sometimes brings even the most skull-shattering sound to a halt? Snoring can be caused by the architecture and muscle tone of the structures in and around the pharynx, which is made up of the nasopharynx, oropharynx, or laryngopharynx (Figure 6.1).1 During sleep, the waking-state muscle tone is lost and this tissue closes in to varying degrees and vibrates as the breath moves past. There are other locations, such as the nasal passageway or between the lips, that can cause snoring. It often occurs during inhalation but also happens with exhalation. Consuming alcohol, smoking cigarettes, or having nasal congestion from a cold worsens snoring, as can being overweight or pregnant. While some snorers have no idea they are snoring and will swear, “I never snore,” others will awaken themselves with the noise. Heavy snoring might be an indication of obstructive sleep apnea, but not always. Because of the potentially lethal consequences of obstructive sleep apnea, if a heavy snorer is also sleepy during the day, it is important to consider a sleep study to rule out apnea. This path of preventative medicine may save the snorer’s life.
Figure 6.1 Mouth and pharynx
Treatments for snoring include side sleeping, losing weight (if overweight), eliminating nicotine, and avoiding or reducing alcohol. There are also many devices that can help, from inexpensive over-the-counter gadgets to costly oral appliances designed by dentists trained in sleep medicine. The range of efficacy of these devices is broad, with the same device working well for one person and not at all for another.
One of the populations overlooked in regard to sleep disorder–related breathing is children, even though up to 15 percent of them may have it. It is disconcerting that 90 percent of such cases are undiagnosed. It can be associated with headaches, irritability, bedwetting, and of course, daytime sleepiness. Causes range from problems with tonsils to irregular facial bone development, so engaging a pediatric otolaryngologist (ear, nose, and throat physician) can be impactful.
Obstructive Sleep Apnea
The statistics surrounding obstructive sleep apnea (OSA) are alarming when we consider it occurs in more than one in four adults between thirty and seventy years old, with over 80 percent of cases undiagnosed. If a risk factor such as having posttraumatic stress disorder or being overweight is added to the equation, the likelihood of having OSA increases dramatically. OSA can cause diabetes, weight gain, stroke, heart attack, high blood pressure, and depression, so we must increase education and screening for OSA. But what is OSA exactly? The airway is obstructed during sleep, and the oxygen levels in the body and brain drop, with associated damage to tissue depending on the severity of the disorder. If oxygen levels drop low enough, small parts of the brain and the heart could die each night. The reason airflow gets blocked is usually because the tissue of the throat or the weight of the tongue closes off the opening in a manner more extreme than snoring. Snoring allows the air to pass through, despite the vibration of the tissue. In contrast, with OSA, the air is blocked for a varied amount of time, happening a few or hundreds of times each night, often without the sleeper having any idea. Heavy snoring can be an indication of OSA, but also people who do not snore at all might still have OSA. Waking up with headaches, feeling sleepy during the day, and having cognitive decline or unexpected weight gain are all OSA symptoms. OSA is diagnosed with a sleep study, and now there is also at-home equipment that can be used in many cases, making it even easier to take this crucial step to improve health.
Once OSA is diagnosed, there is an assortment of choices for treatment, including weight loss (if a person is overweight), quitting smoking and/or drinking alcohol, sleeping with an apparatus to keep the person on their side, and using oral appliances or devices that keep the airway open with air pressure. Continuous positive airway pressure (CPAP) consists of a piece that goes over the mouth and/or nose connected to a hose that supplies a flow of air to keep the airway open. There is an array of shapes and sizes, so if a patient is not comfortable wearing what they are given, it is important that they advocate for themselves to get a more comfortable device (Figure 6.2). There are also oral appliances that can hold the tongue or move the jaw forward, and these do not rely on an airflow machine. Some patients resort to surgeries, but they are typically not as effective as CPAP. Visit this Harvard Medical School website2 for apnea resources and a video of retired basketball player Shaquille O’Neal going through the process of being diagnosed and treated for his OSA.3
Figure 6.2 Continuous positive airway pressure (CPAP) consists of a piece that goes over the mouth and/or nose
Central Sleep Apnea
Central sleep apnea (CSA) is a rare disorder compared to OSA and is associated with the brain not sending the signal to breathe.
Some cases of CSA are caused by problems with the heart or kidneys or from taking opioids for longer than two months. The concept of CSA is similar to OSA in that the person will be tired during the day because they are not receiving enough oxygen when sleeping, but treatments will vary depending on the cause.
Figure 6.3 Hā
Sudden Infant Death Syndrome
Sudden infant death syndrome (SIDS) is not a sleep disorder per se, but it is worthy of discussion in this chapter. SIDS is the sudden, unexplained death of an infant younger than one year old and is the leading cause of death in children one to eleven months old. The highest rates are in babies two to four months old. Research suggests it is linked to an abnormality in the brainstem. Studies are underway to further investigate the possibility of a hearing screening test to identify babies at increased risk of SIDS. The connection may be the hearing pathway traveling through the brainstem. While the cause of SIDS is not known, certain practices increase the risk and so are best avoided: inhaling secondhand smoke, sleeping on soft surfaces, overheating, or sleeping on the stomach. The current advice is to put babies on their backs to sleep, use a firm mattress, and put babies in sleep clothing or a sleep sack so covers are not necessary (Figure 6.4). Breastfeeding has also been shown to dramatically reduce the risk of SIDS.
Figure 6.4 Back to sleep
Restless Legs Syndrome
Having restless legs might not sound too bad, but with an increased risk of depression and anxiety, as well as the myriad consequences of poor sleep, restless legs syndrome (RLS) has far-reaching repercussions on a person’s life. This arises from what is often an indescribable sensation—perhaps tingling or itching—that triggers an overwhelming urge to move the legs. The sensations tend to disrupt daily activities, such as riding in a car or sitting in a classroom, and they are deleterious to sleep.
Sometimes the cause is unknown, but anemia, diabetes, or pregnancy could give rise to RLS or make it worse. Medications such as antidepressants, allergy medications, over-the-counter sleep drugs, and antinausea medications can cause and aggravate RLS.
Exercise may relieve the symptoms of RLS, but interestingly, exercising with too much intensity can increase them. Stress-reducing and muscle-relaxing practices such as yoga, meditation, warm baths, and massages mitigate the symptoms and promote sleep. Eliminating nicotine, alcohol, and caffeine is crucial.
Periodic Limb Movements
Occasionally people confuse periodic limb movements (PLM) with RLS, but they are separate disorders. While RLS sensations cause the urge to move the legs, PLM is an unconscious and uncontrollable movement itself. The big toe or leg moves a couple of times a minute for up to an hour. Sometimes, though rarely, movements are also in the arms. These common leg movements often do not disrupt the sleeper and, if that is the case, would not be considered a disorder. In fact, a sleeping partner is the one who may have their sleep disrupted, while the person with PLM is snoozing peacefully. If the movements do disrupt the sleep of the person with PLM, at that point, it is considered a disorder and will have all the consequences of poor sleep.
Sleep Leg Cramps
Almost everyone will experience sleep-related leg cramps at least once in their life, but some individuals have several of these intense and painful muscle contractions every night. Both the cramp itself and the lingering pain make it difficult to sleep. Sleep leg cramps are more likely in the presence of diabetes, dehydration, electrolyte imbalance (including potassium, calcium, or magnesium), diuretics, and some medications. While strenuous exercise is sometimes listed as an aggravating factor, the association might be more about a lack of rehydration, stretching, or electrolyte replacement after the strenuous exercise rather than the exercise itself. In most cases, daily exercise, including stretching, helps prevent leg cramps (Figure 6.5). In addition to a daytime exercise program, light exercise—like a walk or gently riding a stationary bike—for a few minutes before bed can fend off cramps. During the cramp itself, stretching, walking, massaging, and heat provide relief. Health-care practitioners are able to determine if there are imbalances (such as an electrolyte imbalance) or other medical conditions that, when treated, will resolve the leg cramps.
Figure 6.5 Stretching
Bruxism
Strongly clenching the jaw or grinding the teeth during sleeping or waking states is called bruxism. As a sleep disorder, the episodes happen from a few to hundreds of times each night. Depending on its severity, bruxism can damage teeth, disrupt sleep, and lead to headaches or pain similar to an earache. In many instances, people who have bruxism are wholly unaware. Risk factors are stress, anxiety, anger, frustration, extreme competitiveness, hyperactivity, medications (including antidepressants), nicotine, alcohol, caffeine, and some mental and physical health disorders (such as gastroesophageal reflux disease). To aid in resolving bruxism, consider cognitive behavioral therapy (for anxiety, stress, etc.) and relaxation strategies such as mindfulness, meditation, and yoga, as well as addressing the risk factors. Oral appliances—similar to mouth guards—protect the teeth during sleep but do not address the disorder.
Sleep Paralysis
Since it is normal to be paralyzed during REM sleep, “sleep paralysis” does not sound like a disorder, but it is. Perhaps it should be called “presleep paralysis” or “postsleep paralysis” because those are the times it occurs. An episode of a few seconds or minutes may happen several times a year or only once in a lifetime. A person is unable to speak and cannot move except to breathe and move their eyes. Most of the people I have worked with who have sleep paralysis have reported visual hallucinations, such as seeing a person at the foot of the bed, and also feelings of anxiety during the episode (Figure 6.6). Being sleep deprived or stressed or having an irregular sleep schedule increases the likelihood of having sleep paralysis. It is also associated with particular medications, narcolepsy, and psychiatric conditions, including bipolar disorder. Other than ruling out and addressing mental or physical health problems and narcolepsy, the treatment usually involves attending to stress and getting regularly scheduled eight-hour sleep sessions each night. To reduce their anxiety, I have coached people on meditation and breathing techniques to use during the paralysis. They have all reported to me that the practice makes them feel less aversive and fearful of the episodes, and consequently, their sleep quality improved.
Figure 6.6 Sleep paralysis hallucination
REM Sleep Behavior Disorder
When the normal paralysis of REM sleep does not take over, a person will act out their dreams by jumping, shouting, swinging their arm, or whatever happens to be taking place in the dream (Figure 6.7). This is REM sleep behavior disorder (RBD). Unlike sleepwalking, a person with RBD will usually have their eyes closed and rarely walk. Upon awakening, they swiftly become alert and are able to report their dream, which will contain activities that match their observed movements. This can happen four times a night, every night, or as rarely as once a month. The sleeper does not have awareness of the episode. Alcohol use (and withdrawal), certain medications, and sleep debt exacerbate RBD. Because more than one in three people with Parkinson’s disease also have RBD, health-care practitioners recommend monitoring RBD patients for signs of Parkinson’s so early treatments to slow the course of the disease can begin immediately. RBD patients are also at greater risk of experiencing other sleep disorders, such as narcolepsy and sleep apnea, so they require regular sleep studies so these other disorders can be diagnosed and treated. RBD itself is usually treated with medication.
Figure 6.7 Falling asleep
Sleep-Related Eating Disorder
Getting up in the middle of the night for a snack might sound harmless, but that is not the only thing happening with sleep-related eating disorder (SRED). In this case, the person will typically binge eat quite rapidly and, since they are not completely alert, could cut or burn themselves cooking. The foods they eat are also sometimes inedible items such as raw meat, coffee grounds, or even cleaning supplies (Figure 6.8). Unlike a sleepwalker, who will likely be scared if you awaken them, a person with SRED tends to be angry and hostile when aroused from an episode. They may or may not have any memory of the event, so it can be frightening to arise in the morning to a messy kitchen and a stomachache. Using antidepressants, sleep prescriptions, and other drugs can cause SRED. Getting poor sleep increases the frequency of these episodes. Typically, a doctor will prescribe medication to treat the symptoms.
Figure 6.8 Midnight snack
Sleepwalking
During slow-wave sleep in the first half of the night, a person may walk, or sometimes run, out of bed, with glazed-over and open eyes (Figure 6.9). They talk or engage in other behavior, sometimes elaborate and/or inappropriate. Episodes can occur just a few times in a year or several times each night, or even during a nap. Awakening someone from sleepwalking can be very scary and disorienting to the sleepwalker. While it is a myth that it is dangerous to awaken a sleepwalker because they may die from the fright, it is in fact dangerous to awaken a sleepwalker too suddenly because, in their confusion, they may attack and hurt you or themselves. If you feel completely comfortable, gently guide the person back to bed, touching them as little as possible, coaxing them in the right direction until they get into bed themselves. That approach is risky, so the other option is to get a safe distance away and make a noise, gradually increasing in volume, until the person awakens. They will startle, but at least you are out of harm’s way. Then gently explain to them that they are all right and were sleepwalking.
Figure 6.9 Sleepwalking can be dangerous
Alcohol, sleep prescriptions, stress, irregular sleep schedule, posttraumatic stress disorder, asthma, premenstrual syndrome, fever, certain drugs, and sleep debt can cause sleepwalking. Mindfulness, meditation, hypnosis, and stress-reduction strategies can treat it. It is also important to do a safety check in the bedroom and home to minimize the harm that may come during an episode. For example, make sure the sleepwalker will not have easy access to prescription drugs, scissors, or car keys, and put gates across stairways.
Now that you are familiar with sleepwalking, take a moment to compare it to REM sleep behavior disorder.
Bad Dreams, Nightmares, and Night Terrors
It is normal to have an occasional “bad dream,” slightly distressing in its feeling. However, when a dream is so upsetting that it causes you to wake up, it is called a nightmare (Figure 6.10). On their own, nightmares are not a sleep disorder unless they occur so often that they are making you lose sleep. One of the difficulties is that since nightmares occur during REM sleep, the dream is vivid, so upon awakening, and even throughout the next day, it can be a challenge to clear it from the mind.
Figure 6.10 Nightmares
In contrast, when aroused from a night terror, which usually occurs during slow-wave sleep, with its associated dull dreams, there is usually no memory of the dream. However, there is nothing dull about the physiological response to night terrors. A person awakens from a night terror with an overpowering sense of fear and a pounding heart, shaking and perhaps even screaming, jumping out of bed, or striking out at someone. They are also usually disoriented and slow to respond to someone trying to soothe them. Night terrors are typical during the first third of the night, when we have the most slow-wave sleep, while nightmares usually occur during the latter third of the night, during our longer periods of REM.
Nightmares and night terrors have a range of causes including antidepressants, high blood pressure prescriptions, alcohol, posttraumatic stress disorder, exhaustion, mental disorders, and inconsistent sleep schedules. Treatments include addressing these factors as well as implementing stress-reduction and mindfulness practices. Imagery rehearsal therapy is a promising treatment as well and has also helped reduce daytime trauma symptoms (see chapter 5).
Bedwetting
A child might not be able to control their bladder during sleep until they are five years old, so unless there is bedwetting twice or more a week in a child over five years old, it is not considered a disorder. It is crucial that if a child wets the bed, their self-esteem is considered in the parent’s handling of it. In addition to being harmful to the child’s emotional health, shaming them for it is also known to make the bedwetting more severe and take longer to resolve.
If a child has gone six or more months without bedwetting and then suddenly begins again, it could be due to stress, a urinary tract infection, constipation, or another disorder. In elderly adults, bedwetting may occur with dementia, depression, or obstructive sleep apnea. Some forms of diabetes also cause bedwetting. Rarely, hormonal imbalances could cause bedwetting at any age. Normally, antidiuretic hormone (vasopressin) levels rise during sleep to keep the amount of urine produced low enough so the bladder holds it all night. If these levels are too low, the bladder may fill multiple times during the night, so the person would need to wake up repeatedly to go urinate in the bathroom and might eventually be too tired to awaken. Once mental and physical health issues have been ruled out, treatment should focus on minimizing any shame associated with bedwetting combined with behavioral therapies such as enuresis alarms and positive reinforcement.
Jet Lag
Traveling across time zones can be ruinous to your sleep schedule. You may find yourself waking up in the middle of the night, wide awake and with no ability to go back to sleep, and during the daytime, you may get hit with a strong and sudden wave of uncontrollable sleepiness (Figure 6.11). For many people, it takes one day for their circadian rhythm to shift one hour, so in the days before a trip, try shifting your bedtime closer to that of your destination. Stay hydrated and avoid or have only minimal caffeine and alcohol during the flight. Consider incorporating bright light in the morning or early evening, depending on the direction of the shift; daily exercise; and scheduled fasting. Some people find melatonin supplementation shortly before bedtime on the night of arrival or at the beginning of a red-eye flight to be helpful. Be cautious, and seek advice from your health-care practitioner regarding melatonin because it interacts with some medications and natural remedies. Also, researchers have found that some melatonin supplements carry dangerously high levels of the hormone (many times higher than what is stated on the bottle), and some products labeled “melatonin” contained no melatonin at all.4
Figure 6.11 Can’t sleep
Short Sleeper
Research suggests there is a genetic difference that changes the sleep need of a rare few—less than 1 percent of the population—so they need less than six hours of sleep a night. They never sleep longer than six hours, even on weekends, and they do not need naps. Every morning, they wake up feeling refreshed; they do not have any drowsy periods during the day and so do not need caffeine or any stimulants to stay alert. This sleep pattern begins in childhood, lasts throughout life, and tends to be accompanied by other characteristics like a generally upbeat mood, less of a reaction to painful stimuli, and a somewhat manic personality. It is not possible to teach yourself to be a short sleeper, and if you need to sleep in on weekends, wake up less than revitalized, feel drowsy during the day, or need caffeine to stay alert, you are not a short sleeper. Most people who sleep less than eight hours a night are sleep deprived and are causing harm to their bodies and minds.
Delayed or Advanced Sleep-Wake Phase
There are two separate disorders, delayed sleep-wake phase (DSP) and advanced sleep-wake phase (ASP), categorized as circadian rhythm disorders (see chapter 3). Someone with DSP might refer to themselves as a “night owl” or “night person” because their tendency is to stay up late and get up late. A “lark” and “early bird” refers to those with ASP, who go to bed early and are up before dawn (Figures 6.12a and 6.12b). If someone with either DSP or ASP is able to follow their natural rhythm and still sleep eight hours peacefully each night, their disorder may not cause problems in their life and require no treatment.
If the person’s schedule does have to be changed—for example, due to school, family, or work commitments—research indicates that the use of melatonin, guided by a sleep specialist, is effective in shifting the sleep schedule. Bright-light therapy is also effective for both DSP and ASP, though with inverse timing. For DSP, bright lights and blue light from devices should be avoided in the two hours before one’s desired bedtime, and bright-light exposure (sunlight, if available) should be sought at the time one wishes to wake up. For ASP, light should be avoided in the morning, and sunglasses are recommended for those commuting in the bright morning sun. Then, in the afternoon and early evening, exposure to bright light is important. Because sleep quality is disrupted if DSP and ASP schedules are shifted, cognitive behavioral therapy for insomnia is helpful (see chapter 1).
Figure 6.12a OwlFigure 6.12b Lark
Narcolepsy
Some films use narcolepsy as a joke, depicting those afflicted as having a sleep attack, suddenly falling asleep midconversation. I try to counter this in my classroom by humanizing narcolepsy, showing students interviews with people who have this disorder to demonstrate that it is debilitating and difficult, not funny at all. At my campus of around eight thousand students, I tell those in my classroom to look at the faces of their fellow students and know there could be four students on our campus suffering from narcolepsy, which affects one in every two thousand people. I have had several students with narcolepsy in my classes, and their stories inspire me. They have shared how they have coped and become outstanding students, pursued their academic dreams, and helped people in our communities.
The most notable symptom of narcolepsy is extreme daytime sleepiness—indeed, sometimes sleep attacks (sudden onset of sleep)—that may be accompanied by cataplexy, a loss of muscle tone. Cataplexy can be subtle, such as difficulty with speech, or as severe as total paralysis, causing the person to drop to the ground, sometimes causing serious injury. A person with narcolepsy might not be completely alert when they are going through their day—for example, while in the classroom, talking to someone, or reading a book—and thus may face memory problems as well.
Treatments for narcolepsy involve various medications and prescribed sleep schedules, including naps at regular times during the day. Exercising and avoiding alcohol, nicotine, and drugs are also helpful strategies.
Clinical Sleep Study
Once a person has gone through the Sleep Wellness Guide (see chapter 1) and put in place as many of its strategies as they can, if they are still experiencing daytime drowsiness, it is vital that they consider a clinical sleep study to rule out a sleep disorder. As we’ve seen throughout this chapter, untreated sleep disorders can lead to serious mental and physical health consequences. Thankfully, most insurance companies cover sleep studies, and the experience itself is not unpleasant: most places have created comfortable and private sleeping spaces that feel like a nice hotel (other than the tiny wires placed on your head and in a few places on your body).
That being said, there is one especially troubling thought: Who has insurance, and of those who do, who can afford the copay? If we know sleep debt causes strokes, heart attacks, Alzheimer’s, diabetes, obesity, depression, and more, then whoever cannot afford to fix their sleep is at a huge disadvantage in terms of their health, which should be a basic human right—especially in countries like the United States, where there is access to excellent medical treatment . . . for those who can afford it. I encourage you to consider how you can help bring sleep wellness education and access to clinical sleep studies to everyone who needs it.
1 See also Capital Otolaryngology Head and Neck Surgeons, “What Causes Snoring and Obstructive Sleep Apnea?,” YouTube video, accessed May 5, 2021, https://www.youtube.com/watch?v=i5p0I-Jvtss.
4 Madeleine M. Grigg-Damberger and Dessislava Ianakieva, “Poor Quality Control of Over-the-Counter Melatonin: What They Say Is Often Not What You Get,” Journal of Clinical Sleep Medicine 13, no. 2 (February 2017): 163–65, doi.org/10.5664/jcsm.6434.