How would you react if you saw your bus driver, your surgeon, or your pilot drinking cocktails while performing their job? You would be appalled. Yet sleepiness can be worse than drunkenness in terms of its likelihood of causing an accident (Figure 7.1). Researchers have shown that sleep-deprived individuals drive more recklessly (hit more cones in driving courses) and have worse coordination and reaction time than those who are drunk. Sleepiness in fact causes as many deaths and injuries from car accidents as drunk driving. Those numbers are probably lower than they should be, since highway patrol officers do not have a test for sleep debt and also because people are often unaware of their degree of sleepiness. People can experience four seconds of sleep while driving, performing surgery, flying a plane—you name it—and not realize they are asleep. It is chilling to combine this information with the fact that one in three Americans admits that at least once in the previous month, they have put themselves in the driver’s seat even though they were finding it challenging to keep their eyes open. More than 40 percent of adults report that they rarely or never get enough sleep on weeknights. If legislators could see the deadly effects of drowsiness the same way they see those of drunk driving, perhaps we could motivate them to support an effective educational and health-care movement to address our national sleep debt emergency.
Figure 7.1 Sleepy driving causes as many deaths as drunk driving
Economics
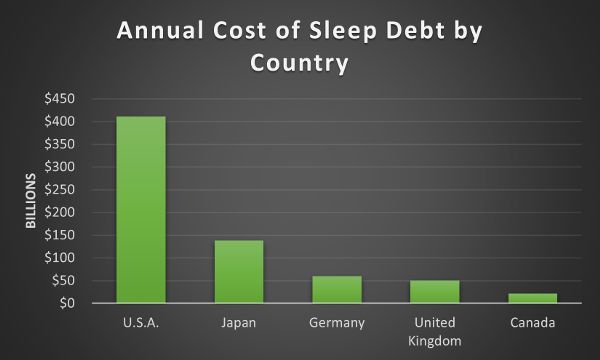
An effective approach may be to talk to people about the financial cost of sleep debt. One of my mentors in social justice and antiracism work told me, “We do this work because we know it is the right thing to do, but if we can show leaders how making these changes is a way for them to save or make money, then we get their attention.” What is the financial cost of sleep debt? $411 billion annually for the US. This comes from a RAND Corporation 2016 report that also listed the annual cost of insufficient sleep for Japan ($138 billion), Germany ($60 billion), the United Kingdom ($50 billion), and Canada ($21 billion) (Figure 7.2).1 If loss of life is not enough reason to justify the allocation of resources for sleep wellness education, saving hundreds of billions of dollars each year should do it.
Valiant efforts have been made to help change attitudes toward sleep in the US. William Dement, known as the father of sleep medicine, dedicated decades to the cause, in particular from 1991–94, when he served as chair of the US Congress–mandated National Commission on Sleep Disorders Research. Yet still, we find our country to be, in the words of US senator Mark Hatfield, a “vast reservoir of ignorance about sleep, sleep deprivation and sleep disorders” (Figure 7.3). It may surprise you to know that Hatfield made this remark all the way back in 1993, and yet sleep debt–related tragedies have been multiplying ever since.
Figure 7.2 Sleep debt by countryFigure 7.3 US Capitol
Antiracism
As we consider the need for action to address the issue of sleep debt, we should keep in mind race-associated inequities in sleep wellness. Is healthy sleep a luxury, afforded only to “non-Hispanic whites”?
Before moving on, it is important to clarify that race is a social construct. There is no biological or anthropological evidence that humans come from different races. We are one race: the human race (Figure 7.4). But race labels, such as Black, are a part of this discussion due to the research, in which they are used to create groups for data analysis. Sometimes, these groups have to do with ancestry, such as in the case of Alaska Natives, so some of these terms are mixed into this section, depending on the studies being cited.
The US Centers for Disease Control and Prevention analyzed data from over four hundred thousand adults and found the prevalence of healthy sleep duration to be significantly lower in Native Hawaiians / Pacific Islanders, non-Hispanic Black people, multiracial non-Hispanics, and American Indians / Alaska Natives compared to non-Hispanic whites, Hispanics, and Asians. This study is just one of several that have provided evidence that there is racial inequality in sleep wellness. Harvard researchers reported that Black participants are five times more likely to have insufficient sleep compared to other groups. Even when socioeconomic status is factored out, the Black participants still get less sleep.2 This has enormous implications when we consider which groups have the highest rates of diabetes, obesity, high blood pressure, and other sleep debt–related disorders. For example, if Blacks and Native Hawaiians, two groups with higher rates of those disorders, are getting poor sleep, and we know poor sleep can cause these disorders, we have an extra layer of responsibility to address the racial inequalities around sleep health.
Figure 7.4 One race: The human race
It is important to point out that the scientific community agrees that there are no innate biological reasons for the sleep differences based on race. Researchers suggest the experience of racism, even in its subtlest forms, impacts a person’s ability to sleep well and, in particular, to enter the deep and restorative sleep of NREM 3. This likely plays a role in the poor sleep reported by those experiencing discrimination based on sexual orientation as well, so consideration for sleep equity must go beyond race, to all groups experiencing discrimination and oppression. It makes sense that sleeping deeply would require the mind to be in a state of ease, knowing we are safe and free. The situation is exacerbated by the reported connection between lack of sleep and reduced opportunity for civic engagement, such as being able to safely and conveniently vote. Insufficient sleep is associated with reduced political participation and decreases in other measures of social capital (Figure 7.5).
Thus sleep inequality research adds one more justification, on top of the mountain of reasons, for fighting racism. It also illustrates the importance of developing targeted sleep wellness education and health services for these groups.
Figure 7.5 Kapu Aloha. Find your cause and speak out!
Business
Company leaders are in a strong position to make their mark, and increase profits, by addressing employee sleep debt. One study of four large companies in the US determined sleepiness was costing them—in lost productivity alone—around $3,000 annually per employee. For the four companies in the study, the yearly capital loss was over $50 million. On a national level, poor sleep causes on average, per person, eleven days of lost productivity in the US. In the United Kingdom, one in five workers report that they had recently arrived late to work or skipped work due to insufficient sleep. More than one in four employees in Canada take sick days because of sleepiness. Sometimes the reason we don’t get enough sleep is because we are staying at our jobs late into the evening in hopes of completing more work. The irony is that if we are low on sleep, it will take us longer to finish the work because of decreased cognitive and physical functioning. We, and our companies, would be better served to call it a day, get a good night’s sleep, and start new in the morning. But first, a company must develop a prosleep culture that supports this wise decision-making.
In Japan, as part of a response to survey results indicating that 90 percent of adults do not get enough sleep, some companies are paying their employees to sleep. One Japanese company uses a phone app to record hours of sleep, and if the employee reaches the target, they earn points to use for cafeteria purchases. In the US, Ben and Jerry’s, Google, Huffington Post, and Nike have places where staff can sleep while at work (Figure 7.7). Reboot, a marketing company in London, provides a peaceful room for napping. Many companies around the world are seeing the benefit of allowing their employees to work the hours better matched to their chronotype: for example, letting the night owls start their shift later in the morning. Considering the impact of poor sleep on cognitive function, productivity, accidents, and illness, companies could get an enormous return on their investment by supporting healthy sleep for their employees.
Figure 7.7 Nap pod
High Schools and Colleges
An international comparison found that among the fifty countries studied, the US has the most sleep-deprived students. One in three high school students fall asleep in class, and although teenagers need nine hours of sleep each night, most are sleeping around seven or fewer; less than 10 percent of them are getting enough sleep (Figure 7.8). African American and Hispanic students, as well as those from low-income households, get even less. In Japan, half of high school students are sleeping six or fewer hours on weeknights.
Figure 7.8 Sleeping in class
Adolescent sleep deprivation is an alarming epidemic. The American Academy of Pediatrics, the American Association of Sleep Medicine, and the American Medical Association have all identified insufficient sleep in adolescents as a serious public health issue and recommend that high schools should not start before 8:30 a.m., even though most of them still begin much earlier. Consider the short- and long-term impact of insufficient sleep on teenage mental and physical health, such as increased rates of depression, anxiety, high blood pressure, obesity, and diabetes. Research suggests teen suicide, violence, and accidents are reduced if teens are given the opportunity to get a healthy amount of sleep. In addition to educating families about the importance of sleep, convincing school districts to move to later start times would start a revolution with tremendous and far-reaching impact. Along with higher academic achievement, school officials could boast about reductions in their students’ rates of illness, depression, tardiness, and suicide.
If the traditional school start time is 8:00 a.m. and a student awakens at 6:30 a.m. to get ready and catch a bus, it is almost impossible that the teen could have gotten enough sleep: to get the nine hours most teens need, they would have to be sleeping by 9:30 p.m. Add to the equation their delayed circadian rhythm, a normal physiological part of being a teen, and it is even more unlikely they would be able to pull this off, even under the best of circumstances. For their bodies, the experience of getting up at 6:30 a.m. would be like an adult getting up at 4:30 a.m. every day for work. So it comes as no surprise that schools that shift to a later start time report a reduction in mental and physical health problems, alcohol and drug use, and traffic accidents, as well as increased academic success.
In Japan, Australia, New Zealand, England, and Finland, they have had later school start times for decades, and each of these countries has higher achievement rates than the US on standardized exams. In the fall of 2019, California became the first US state to mandate later high school start times, reflecting its value for its children’s health. Since studies have shown that bus scheduling, after-school programs, student jobs, and sports activities are not affected by later start times, hopefully more states will follow California’s lead (Figure 7.9).
Figure 7.9 Golden Gate Bridge, San Francisco, California
Get involved in your community by having discussions with local school administrators about the American Academy of Pediatrics 2014 policy statement3 and the Society of Behavioral Medicine position statement,4 which are calls to action, with compelling scientific evidence, for delaying school start times. You can also contact wise politicians such as US congresswoman Zoe Lofgren, who in 2017 introduced the ZZZ’s to A’s Act as a House Bill to “direct the Secretary of Education to conduct a study to determine the relationship between school start times and adolescent health, well-being, and performance.” An easy step for getting involved, and a way to find a range of resources, would be to visit startschoollater.net.
When you were in school, do you remember having lessons about healthy foods and sex education, as well as classes emphasizing the importance of physical fitness? Most people in the US would answer yes. However, what about lessons on the importance of sleep? Let’s encourage our teachers and school administrators to incorporate lessons on the importance of healthy sleep for academic and athletic performance, stable mood, safe driving, and physical health. Getting children and teens motivated to sleep well is a wise place to build momentum for this much-needed sleep revolution.
Students fortunate enough to make it to college are faced with further challenges. With the high cost of tuition and textbooks, there is considerable pressure on college students to work long hours and take too many credits at once to finish school early so they can get a job, leaving only a small amount of time for sleep. In a survey of industrialized nations, with the adult population sorted by age, college-age people get the worst sleep. In Korea, college students sleep on average 6.7 hours per night, and I imagine many college students reading this book wish they could get six hours. The connection between depression and poor sleep, along with the high rates of depression and suicide on college campuses, adds more urgency to the issue. Surveying college students about their sleep is one way to start conversations and increase awareness about sleep debt. This opens the door for us to share resources about how to improve sleep. Illinois State University students made up their faces to look like zombies and walked around campus handing out sleep kits as a part of their “Don’t Become a Zombie” campaign (Figure 7.10). Stanford University has a Refresh program that has been modified and implemented on many other campuses as well, including Dartmouth, the University of Chicago, and the University of Iowa. These programs teach students about the importance of sleep health and provide successful strategies for getting healthy sleep. Several campuses in the US, the United Kingdom, and Japan have also created napping spaces for students. Some have beanbags and others have cots in areas where students sign up for a napping timeslot. Students can reach out to their student government organizations and student health centers for opportunities to provide sleep wellness education activities and find resources to create napping spaces.
Figure 7.10 Zombies
Health-Care Providers
The issue around sleep debt and health-care providers has three components. The first one is foundational: the lack of education on sleep wellness and sleep disorders provided to our doctors and nurses. Studies report that the total amount of time dedicated to sleep education in our doctors’ preclinical training is only fifteen minutes. If they received more education, we could expect a decrease in the current rate of sleep disorders that are left undiagnosed (95 percent).
Figure 7.11 Wana (sea urchin) are a source of healing food in Hawaiʻi
The second component is the lack of sleep-health education and screening provided by health-care practitioners (kahuna lapaʻau in Hawaiian) to their patients.
Primary care physicians should administer a sleep-quality questionnaire and screen patients for sleep problems like how they screen everyone for high blood pressure (Figure 7.12). If a physician sees a patient for something as minor as a splinter, they still have the medical assistant slap on a blood pressure cuff to screen for hypertension (high blood pressure). We need to approach sleep-health screening in the same manner. Every patient should get surveyed; then the survey data should be used as talking points to emphasize the importance of sleep and address any problem areas. Drowsiness should be discussed and pursued. Patients should be asked to keep ten-day sleep diaries and submit those in follow-up appointments. A primary care clinic in Idaho surveyed a little over 1,200 patients who were coming to the clinic for a variety of reasons (besides sleep disorders) and found over 60 percent of them also had sleep disorder symptoms. At that point, all but two of the patients had not been diagnosed. Imagine if we could generalize this type of care and reduce illness, accidents, and deaths related to sleep debt and sleep disorders.
Figure 7.12 Physicians have the potential to play a critical role in sleep wellness
The third and final component is the demanding shift work required of our health-care providers and hospital workers. We must change the guidelines for this because there are too many deaths and accidents clearly documented and linked to health-care provider sleep debt. For example, physicians in their residency (the two to seven years they practice while learning their specialty) are working with such high sleep debt that one in twenty report that they have killed a patient due to errors they made because they had not gotten enough sleep (Figure 7.13). In a survey of residents in a San Francisco hospital, over 40 percent of residents disclosed killing at least one patient due to sleepiness. Stanford University researchers have used the multiple sleep latency test for years on numerous residents and nurses, and according to them, of all those respondents, only one person “was not in the twilight zone of extreme sleepiness.”5 Johns Hopkins released a study in 2016 stating medical errors are the third-highest cause of death in the US, making medical errors the reason for 10 percent of all US deaths.6 Knowing how sleep-deprived medical workers are, it is not a leap to consider lack of sleep playing a part in those medical errors and therefore deaths.
Figure 7.13 MedGlobal volunteer performs surgery at Al-Shifa hospital in Gaza Strip
The medical establishment needs to be held accountable and revise the work schedules of our health-care providers. The National Academies of Science, Engineering, and Medicine gathered a group of medical and scientific experts to examine evidence and propose revised work schedules for medical residents. For example, with these revisions, they would get a five-hour break for sleeping after working sixteen of their thirty hours in a shift. However, the Accreditation Council for Graduate Medical Education (ACGME) has done too little to have much impact, and way too many sleep debt–related accidents and deaths continue to occur. To put it in perspective, in the US, the ACGME mandates that the maximum number of hours a resident can work per week is eighty, but many European countries, whose medical programs still have excellent success rates and train physicians in a similar number of years, set the maximum at forty-eight.7 We need to increase awareness of the tragic number of preventable deaths and injuries associated with the sleep deprivation imposed on our health-care providers and pressure the medical establishment to change.
Your Next Steps
The World Health Organization says we are in the midst of a “global epidemic of sleeplessness.” The Centers for Disease Control and Prevention report that over 40 percent of adults said they had fallen asleep during the day unintentionally at least once in the past month. In the US and Japan, more than 65 percent of adults are not getting enough sleep. The problem is not limited to industrialized societies. A study of people living in rural, low-income communities without the trappings of industry in eight African and Asian countries found that a large number of adults were not getting enough sleep. The authors used their study’s results to urge people to see the global nature of the sleep debt epidemic.8
There are many approaches to resolving this problem and decreasing its associated catastrophes. One place to start is to address the lack of awareness about sleep debt and the dearth of public policies promoting healthy sleep.
Let’s take a glance at previously successful campaigns that had impacts on public health. Thanks to scientific evidence about the dangers of cigarette smoking, we saw the rise of consumer warnings added to packaging as well as designated nonsmoking areas. After learning more about automobile accidents, we went from cars not even having seat belts to passing laws requiring that all passengers wear them. Vaccine awareness and access helped eradicate smallpox and almost eradicated polio and other diseases. Research on death in infants led to the Back to Sleep campaign to reduce the incidence of sudden infant death syndrome. Widespread distribution of posters provided education about reducing the spread of disease through handwashing. We know we can have an impact, and now is the time to act to increase sleep-health education.
After completing my course on the science of sleep, or simply reading this book, you are likely a sleep expert compared to most of the people in your community, so I ask you to take that knowledge and use it to make an impact on your community. You can read the previous sections for ideas, but here are a few more:
• Choose some sleep wellness and sleep disorders information (for potential content, see chapters 1 and 6 in this book) and put it in a format you like—a flyer, brochure, poster, or sheet of talking points—and go with a friend to do targeted sleep-health education in underserved neighborhoods. You might consider visiting a beauty salon, barbershop, church, or school to share your expertise (Figure 7.14). A good way to start the conversation is by asking people to tell you about their sleep and their early evening routines. People usually like to share their stories. Your first step is to encourage dialogue about sleep.
Figure 7.14 Start a sleep wellness conversation at the barbershop
• Get resources from, or provide support to, a nonprofit such as Pajama Program9 and help children get sleep.
• Reach out to educate leaders in occupations known to have increased levels of sleep debt: health-care workers, airline employees, bus drivers, truck drivers, police officers, first responders, and military.
• Visit your campus health center and ask them to consider providing sleep wellness screenings and to discuss snoring, insomnia, apnea, and daytime drowsiness.
• Talk to colleagues at work about their sleep. Identify things at your workplace that could change to support healthy sleep. Approach an ally in a leadership role in your company and discuss the financial gains likely achieved if they adopted a prosleep culture. Ask them to consider creating a safe napping space, providing sleep disorder and insomnia screening, starting a healthy sleep awareness program, and adjusting shift hours based on chronotype.
• Start a petition or grassroots effort to eliminate daylight savings time.
Consider the successful business leaders, school administrators, and politicians mentioned earlier in this chapter, who have chosen to make healthy sleep a priority for large groups of people and achieved much along the way. Please find an arena where you have a natural interest—perhaps a school, a local political group, a veterans club, an eldercare facility, a health clinic for the underserved, your workplace or college campus—and begin a conversation with someone about how to raise consciousness about sleep wellness. Let’s work together to help people get the sleep they deserve so we can bring more equanimity, health, and peace to our communities and beyond.
1 Marco Hafner et al., “Why Sleep Matters—the Economic Costs of Insufficient Sleep: A Cross-Country Comparative Analysis,” Rand Health Quarterly 6, no. 4 (2017): 11, https://doi.org/10.7249/RR1791.
2 Yong Liu et al., “Prevalence of Healthy Sleep Duration among Adults—United States, 2014,” Morbidity and Mortality Weekly Report 65, no. 6 (February 2016): 137–41, http://dx.doi.org/10.15585/mmwr.mm6506a1.
7 Pelayo, Dement, and Singh, Dement’s Sleep and Dreaming, 428.
8 Saverio Stranges et al., “Sleep Problems: An Emerging Global Epidemic? Findings from the INDEPTH WHO-SAGE Study among More Than 40,000 Older Adults from 8 Countries across Africa and Asia,” Sleep 35, no. 8 (August 2012): 1173–81, https://doi.org/10.5665/sleep.2012.